From Star Trek: Theurgy Wiki

Officers within the medical department included medical officers and had the responsibility of maintaining the physical health of all personnel on board their starship or starbase , while also providing physical treatment to civilians that the starship encountered or who visit the starbase . Based out of San Francisco on Earth, Starfleet Medical oversaw all Starfleet medical personnel and facilities, which included exercising co-authority, besides the captain, over starship sickbay personnel. As its emblem, the department carried, from the mid-2150s onward, a stylized version of the double-snaked medical caduceus symbol from ancient Greek mythology. With the launch of the NX-class, Starfleet Medical asserted its co-authority over sickbay, by having its symbol prominently featured on the transparent access doors to sickbay, something repeated two centuries later with the Galaxy-class. In the 2270s and the 2280s (when the emblem was shortly replaced with a variant design), the emblem was worn by starship medical personnel on their garments when on duty in sickbay.
- 1 Mission Status
- 2 Positions
- 3.1 Anesthesiology
- 3.2 Biology/Xenobiology
- 3.3 Dentistry
- 3.4 Emergency Medicine
- 3.5 Imaging Systems
- 3.6 Immunology
- 3.7 Internal Medicine
- 3.8 Medical Toxicology
- 3.9 Neuropsychology/psychiatry
- 3.10 Rheumatology
- 3.11 Surgery
- 4.1 Recovery Ward
- 4.2 Primary Care Unit [PCU]
- 4.3 Intensive Care Unit [ICU]
- 4.4 Medlab 01 & 02
- 4.5 Surgical Suite 01 & 02
- 4.6.1.1 LMH
- 4.6.1.2 EMH Mark I & II
- 5.1 Autosuture
- 5.3 Brain-circuitry Pattern
- 5.4 Cardio-Inducer
- 5.5 Cortical Stimulator
- 5.6 Delta Wave Inducer
- 5.7 Dermal Regenerator
- 5.8 DNA Reference Scan
- 5.9 Exoscalpel
- 5.10 Hyperencephalogram
- 5.11 Hypospray
- 5.12 K-3 Indicator
- 5.13 Medical Kit
- 5.14 Medical tricorder
- 5.15 Micro-Tone
- 5.16 Neural Bridge
- 5.17 Neural Imaging Scan
- 5.18 Neural Stimulator
- 5.19 Neural Transducer
- 5.20 Optical Scanner
- 5.21 Psychotricorder
- 5.22 Retinal Imaging Scan
- 5.23 Sonic Separator
- 5.24 Surgical Support Frame
- 5.25 Tissue Scanner
- 5.26 Trilaser Connector
- 5.27 Vascular Regenerator
- 6.1 Analgesics
- 6.2 Anesthetics
- 6.3 Antibiotics
- 6.4 Burn Treatments
- 6.5 Cardiovascular
- 6.6 Neurological
- 6.7 Radiation
- 6.8 Recreational and Narcotic
- 6.9 Respiratory
- 6.10 Resuscitative
- 6.11 Sedatives
- 6.12 Stimulants
- 7 Disclaimer Notice
Mission Status
This segment describes the current situation aboard the Theurgy .
UNDER CONSTRUCTION
As of 2381, these were the different roles in this department:
Medical Fields
These were medical fields that was interesting for a medical officer, As in real life, there was overlap between different field. Different fields of study and expertise informed one another, and officers may develop similar skills from differing origins.
Anesthesiology
The study of pain management and anesthesia for use during major, invasive medical procedures, as well as therapeutic treatments. This also covered the monitoring patient’s vital signs.
Biology/Xenobiology
The study of biological organisms, and their biological processes is of great importance to medical professionals. Medical officer with this field were extremely knowledgeable in numerous species, both humanoid and not – as well as fauna native to dozens of worlds. This field could often be used to provide background information on a patient’s physiology prior to attempting medical treatment.
This field of medicine focused on treating the mouth, teeth and gums. Advances in personal care had made routine dentist visits effectively painless for most humanoids, however, there was an ever-increasing need for dentists capable of operating on species such as Klingons, Ferengi or Nausicaans.
Emergency Medicine
This field provided the medical officer with in-depth knowledge and training required to make immediate decisions to prevent loss of life or further major medical complications. These individuals were most often found in emergency response groups as well as within the trauma ward of medical facilities.
Imaging Systems
Modern medical science depended heavily on the state-of-the-art imaging equipment that allowed physicians to literally see into a patient’s body and directly identify ailments and damaged tissues. However, there were some individuals that were extremely well versed in the use of this technology and able to obtain information that others couldn't. This field could be used any time an imaging device was used in the course of a treatment, where the quality and clarity of information was of particular value.
Medical officers with this filed were well trained in the body’s natural immune system, including how it identified and reacted to foreign bodies to prevent the spread of infections. In addition, this field also provided the medical officer with extensive understanding of the disorders of the immune system and potential ways to prevent or treat autoimmune disorders.
Internal Medicine
The broad study of internal organs. This field could be used any time the physician was dealing with the diagnosis and treatment of the internal organs – specifically those within the chest and abdomen.
Medical Toxicology
Specializing in the treatment of injuries originating from exposure to drugs and chemicals, as well as biological and radiological contaminates. Further, medical officers with this field were extremely knowledgeable in counter-agents to prevent lasting damage, and may even be able to identify local flora capable of meeting those needs.
Neuropsychology/psychiatry
A sub-specialty that dealt with diseases of the nervous system, especially when it resulted in emotional or mental disorders. Medical officers with this field possessed a strong understanding of both the physical structure of the brain as well as how that drove emotional and thought processes.
Rheumatology
The medical specialty dealing with the diseases of joints, bones, and connective tissues. This field could be used whenever the physician was attempting to determine the cause of recurring pain or identifying degenerative conditions affecting the joints, muscles, and bones.
This field, as its name implies, covered surgical procedures of all kinds and any instance of when the treatment of injuries required surgical intervention. It also covered the tools and equipment required to perform a successful surgery and any particular concerns or issues that may arise when performing surgery on species.
USS Theurgy Sickbay

Sickbay was an old Navy term for "ship's hospital", which continued even into the 24th Century.
Number of Primary Care Biobeds: 12 Number of Intensive Care Biobeds: 8 Number of Recovery Beds: 12 Number of Surgical Beds: 2 Number of Isolation Units: 1 Number of Decontamination Chambers: 2 Number of Medical Replicators: 7 (1 for each area except for the morgue)
Recovery Ward
Pretty much where you'd end up if your illness or injury was not too life-threatening but the doctor required you to hang around overnight for treatment and/or monitoring. Also was where non-critical patients were placed after surgery. Included 12 biobeds with overhead monitors, sanitized pillows and sheets for each bed, 1 replicator, and supply storage cabinet close by.
Primary Care Unit [PCU]
This was most likely where you'd be treated for bumps, bruises, common diseases, and anything else that didn't look to be particularly life-threatening. Included 12 scanning biobeds.
Intensive Care Unit [ICU]
Here's where you'd go if the doctors weren't sure whether you'd die soon or not and there was little more they could do about it but watch and wait. Each biobed was rigged for constant 3-dimensional scanning and monitoring of the patient. Included a computer link-up to an adjustable "Code Blue" alarm system that sounded the instant a patient's life-signs fell out of acceptable parameters. Also included 1 replicator, additional life support hardware for each bed, back-up battery power on a separate power grid from the ship, atmospheric isolation systems, and a supply storage closet that could be found near by.
Medlab 01 & 02
The primary laboratories for Sickbay's use. These included 1 replicator, material diagnostics stations, a centrifuge, gene analysis terminal, a table for post-mortum examinations, and stasis field drawers for storage of biological samples, corpses, or patients requiring treatment not available on the ship.
Surgical Suite 01 & 02
If you needed surgery to save your life, correct an illness, fix a serious injury, or to just have yourself cosmetically altered for an undercover assignment this was where they'd have you laid out. Along with the usual surgical tools, the room included a sanitation module, mobile life support equipment, a replicator, atmospheric isolation systems, and scanning/monitoring readout station.
Battle Sickbays
Because of the Theurgy's MVAM-mode, many main areas of the ship were duplicated, this included the Sickbay. Vector 01 and 03 sections both contained a full Sickbay. Vector 02's Sickbay was the Main Sickbay area [discussed above], while the other two Vectors had one Battle Sickbay each.
Holographic Projection Grid
The USS Theurgy was fitted with the EVE Program AK-1 DMSA-656 , a Long-term Medical Holographic program. She was offline since the first encounter with the USS Calamity , and could only be re-activated after the Battle of Starbase 84 . After the first encounter with the Savi , the LMH's subroutines were compromised and she remained deactivated. She was out of order until her holographic matrix could be repaired.
EMH Mark I & II
In 2371, starship sickbays began to be fitted with holographic technology, allowing activation of a program designed to be a competent doctor, and usable by the crew of the Starship in emergency situations. After rolling the program out on several classes, including the Intrepid and Sovereign classes, Dr Zimmerman designed an updated EMH that he designated Mark II, and was prototyped on the USS Prometheus with holo-emitters enabling it to operate throughout the starship. The improvements to this program were focused on its personality and bedside manner, but retained its medical knowledge and ability at surgical procedures.
The two EMH programs - Mark I and II - were available on the USS Theurgy given the fact that the ship could split into three during Multi-Vector Assault Mode. These programs could be activated to provide additional assistance to the real medical officers. The EMH were programmed with all current medical knowledge and had the ability to learn as required. Additionally, the EMH could take on any other medical role as required by the situation.
Medical Equipment

An autosuture was a handheld unit used to heal reasonably mild wounds to the skin. Autosutures can be used to close incisions or heal knife wounds beyond the ability of a dermal regenerator. In 2369, an autosuture was used to heal a stab wound received by Captain Jean Luc Picard.
The primary biobed in sickbay was designed for surgical purposes, although it was also the default bed for examinations conducted by medical personnel. It had various hookups for surgical equipment, and was typically covered by a large sensor cluster. Surgical beds usually had a large display for vital signs and other information adjacent to the bed. Serious surgeries usually required a larger biobed with more specialized sensors and surgical equipment.
Brain-circuitry Pattern
The brain-circuitry pattern was used as both a medical diagnostic tool as well as a means of identification as such patterns were unique to that individual. The scan created an image capable of mapping the neural activity in the brain.
Cardio-Inducer
The cardio-inducer was a medical device which was used to treat heart conditions in artificial hearts.
Cortical Stimulator
Cortical stimulators helped return the brain and nervous system to a normal, healthy state when a humanoid entered a coma or suffered other forms of serious neurological disturbance.
During treatment, doctors placed the unit on the patient's head. The stimulator's linear array of electromyonic sensors analysed the current level of neural activity and compared this activity to the normal parameters for the patient's species. Using these readings, the physician then activated the stimulator's network of phased muon projectors. Intersecting muon beams focused on individual neurons, stimulating them in patterns similar to normal brain activity. A sufficient level of neural stimulation usually resulted in the patient's other neurons adapting their firing to match this pattern, returning the patient to a normal state.
Doctors would carefully monitor the cortical stimulator or the patient could experience neural damage or seizures. In the hands of a skilled physician this device could even help cure complex neurological abnormalities like the Vulcan t'lokan schism or temporary insanity induced by drugs or stress. Doctors had occasionally used this device to reinforce normal neurological patterns to such a degree that noncorporeal beings inhabiting patients were expelled. On rare occasions when a patient's bioneural energy was temporarily displaced from the body, a cortical stimulator could keep the patient's body alive until this energy was returned.
Delta Wave Inducer
Physicians throughout the Federation used delta wave inducers to help patients enter a deep and restful sleep. Starfleet cadets and other students sometimes used inducers to get to sleep before an important performance review. Most humanoid brains oscillated in a certain range of resonance frequencies (known as delta waves) while asleep; this device artificially induced this state and eased the subject into sleep.
The delta wave inducer was a partial headband that fit comfortably over the user's forehead and temples. The device activated a series of superconducting nickel-rhombium zeta-meson projectors. The zeta-meson fields produced by the delta wave inducer oscillated in the same frequency as delta waves, and caused the neurons in the user's brain to fire in a similar pattern through mesonic induction. Within five minutes of activation, the user fell into a sound sleep. Normally, the unit turned itself off after ten minutes, although a physician could program it to keep the user asleep for a set period of time, waking him up by damping out the delta waves in his brain. Doctors advised healthy subjects who simply needed help getting to sleep not to use this unit more than twice a week to avoid psychological dependence.
Dermal Regenerator
A dermal regenerator was a common medical device used to heal minor wounds although major, gaping wounds and surgical incisions still required an autosuture. The dermal regenerator could also be used for cosmetic surgery such as removing scars as well as removing disguises created through the use of synthetic skin.
DNA Reference Scan
A DNA Reference Scan was a medical procedure to identify an individual by matching the DNA patterns with those on file.
Sometimes internal injuries or the presence of foreign bodies inside the patient required physicians to perform surgery. Based on principles similar to those used by multipurpose gravitonic effectors, exoscalpels were the 24th century surgical cutting device. This unit used trionic emitters to tightly focus a low-powered rapid nadion cutting beam.
Exoscalpels had two modes of operation. In the normal mode, a exoscalpel projected a linear nadion beam that functioned as an exceedingly thin blade. A surgeon could focus the beam as short as 0.1 cm or as long as 20 cm for exceptionally deep incisions. The trionic emitters could also focus the nadions at certain points along the beam. Since only focused nadions could slice tissue, a exoscalpel could cut deeply within a patient without actually piercing the skin or damaging any tissue between the exoscalpel and the affected region. This focused cutting area could extend up to 20 cm away from the unit and could focus as short as 0.1 cm or as long as 5 cm. If the surgical procedure required it, a strong electric charge carried by the trionic beam could instantly cauterize any incision this device made.
Like many instruments, exoscalpels had alternate uses. While this device was incapable of affecting refractory materials like tritanium or Duranium, an exoscalpel could easily cut all ordinary organic material like wood or bone, and most of the boronite whisker composites used in furniture and clothing.
Hyperencephalogram
A hyperencephalogram was a medical test involving an instrument capable of recording and measuring brain-wave activity.
A hypospray (colloquially, hypo) was a medical device used to inject liquids into the body. The system used a non-invasive transport mechanism of compressed air to transfer the injectant from the device into the body without the use of a needle, ensuring that the skin was not punctured during use, thus reducing the risk of infection. Various drugs could be used, inserted into the hypo in vials attached to the end of the instrument.
The 23rd century Federation hypospray resembled the intravenous needles of previous centuries, whilst the 24th century version of the device was more compact, employing an angled head and rounded tip to transfer the drug more easily. Controls at the injection head set the dosage to be injected.
The typical injection site used was the side of the neck, but the hypospray could inject even through clothing. Unlike hypodermic needles, the hypospray could be used on multiple patients without worries of spreading blood-borne illnesses.
K-3 Indicator
A K-3 Indicator was a medical diagnostic device on Starfleet biobeds that measured the neural activity which corresponded with the level of pain as it was being experienced by the patient.
Medical Kit
Medkits, also known as medikits, were pouches used by Starfleet medical practitioners and officers that contained medical equipment for away teams, containing a medical tricorder , a hypospray, a dermal regenerator, and a trauma kit for emergency medical situations. They were often kept in strategic positions around Starfleet vessels and bases.
Medical tricorder
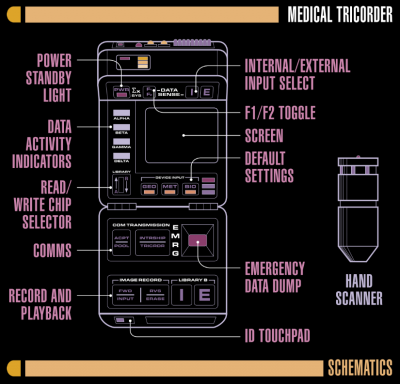
The medical tricorder was a specialized version of the standard tricorder . It was equipped with sensors and analysis software tailored for medical diagnostic purposes. They were usually the first tool a Starfleet doctor utilized when assessing a patient's condition. Medical tricorders could function aboard ship in sickbay as well as on away missions.
A micro-tone was a device which could be used to make extremely precise cuts, such as trying to sever the spine, where a exoscalpel or sonic separator would create too coarse an incision.
Neural Bridge
The neural bridge was a medical device that could be used to stabilize the neural functions of a patient with heavy brain damage. It allowed the brain of a normal person to be used to support a damaged brain.
Neural Imaging Scan
The neural imaging scan was a medical diagnostic scan employed to test acuity of a patient's visual cortex.
Neural Stimulator
A neural stimulator was a medical instrument used to increase activity in the central nervous system of a dying humanoid brain.
Neural Transducer
Neural transducers were small devices used to restore mobility to physically disabled individuals. They could pick up the neural signals from the brain and then stimulate the appropriate muscles. The implants were generally not one hundred percent effective, but did allow a patient to recover most mobility. Motor assist bands were first used to train the patient's nervous system before surgery.
Optical Scanner
The optical scanner was used to perform diagnostics on the visual receptors by Engineering Officers. It could detect phase variances and alterations in the surrounding dekyon field.
Psychotricorder
A psychotricorder was a Federation instrument, similar to a tricorder , used to record past memories.
Retinal Imaging Scan
A retinal imaging scan enabled the Medical Officer to verify the presence or absence of visual cortex activity.
Sonic Separator
The sonic separator was a medical instrument commonly used to separate tissue, similar to a laser scalpel.
Surgical Support Frame
A key part of any surgical operation was the Surgical Support Frame or SSF, which was an attachable device to a Federation biobed. It was commonly called a "clamshell", given its shape and the fact that it was mounted over a patient during a surgical procedure. The SSF provided both a sterile environment and vital diagnostic and life support tools, such as a defibrillator and a pulmonary scanner. The frame incorporated a battery of bio-function sensors to supplement those of the biobed and overhead sensor clusters.
The SSF was capable of automated administration of intravenous medication as well as cardiovascular support and emergency defibrillation.
There were a variety of support frame types for different procedures and different body lifeform types. They were integral parts of any Surgical Bay.
Tissue Scanner
A tissue scanner was used to measure the rate of cellular decay. It could run scans at the molecular level, and was capable of picking up tetryon particles. The sensitivity could be boosted with an enhanced resolution mode, and could adjust the scan field as needed. The unit interfaced with remote computer systems, which could be used to control all functions.
Trilaser Connector
The Trilaser connector was a medical instrument used to reconnect nerve connections.
Vascular Regenerator
A vascular regenerator was a medical instrument used to repair blood vessels and stop bleeding without invasive surgery.
Drugs and Medicines
Asinolyathin : A pain reliever and muscle relaxant. It is used primarily to treat muscle spasms and pain from muscular injuries.
Bicaridine : A strong, addictive, pain reliever used to treat pain from traumatic injuries such as disruptor blasts. Is a known substitute for Metorapan.
Hydrocortilene : A pain reliever used primarily for cranial pains. A dose of 3% is sufficient for a mild headache, whereas increased doses were necessary for more debilitating injuries, such as concussion.
Metorapan : A formidable pain reliever used to treat more severe injuries. It is very similar to bicaridine, though without the risk of addiction. However it can cause fatal allergic reactions in around 1% of cases.
Morphenolog : A medication used primarily in the treatment for chronic pain. It can also be used in conjunction with other medications to reduce painful side effects.
Terakine : A pain relieving medication used to ease the pain from broken bones and similar injuries.
Triptacederine : A potent pain reliever used to aid with end-of-life pain. Another common application of the drug can be to ease the discomfort caused by malfunctioning cybernetic implants.
Anesthetics
Anesthizine : A fast-acting anesthetic typically deployed in a gaseous form. It was considered to be one of the best in use by the Federation .
Anetrizine : A local anesthetic deployed through a hypospray, typically used to numb specific nerves to remove sensation and induce paralysis.
Axonol : A gaseous anesthetic authorised for use by the Federation as a crowd-control measure.
Neurozine : A gaseous anesthetic that was fast acting and could be dispensed through the typical environmental control systems on a Federation Starship.
Antibiotics
Corophizine : An antibiotic used primarily in order to prevent secondary infections.
Burn Treatments
Dermaline : A drug typically administered as a pre-emptive injection when there was a risk of exposure to high level UV radiation.
Dermaline Gel : A thick white gel made from dermaline compounds that could be used to soothe and treat first and second degree burns.
Kelotane : A drug typically administered via hypospray that was used to treat severe burns that were caused by high levels of harmful radiation.
Cardiovascular
Adrenaline : A hormone and neurotransmitter that can be used to prevent anaphylaxis.
Alizine : A medicine used to counteract anaphylactic shock, specifically in Klingons .
Anticoagulant : A medicine administered to prevent or reduce the clotting of blood.
Cateline : A drug that could cause a simulated anaphylactic shock when administered.
Chloromydride : A strong cardiostimulant that was most commonly used when inaprovaline was ineffective. One application was to aid a patient undergoing cardiac arrest.
Cordrazine : A strong stimulant, primarily used to stimulate the heart during cardiac arrest.
Digoxin : A drug administered via hypospray that could be used to treat atrial fibrillation, atrial flutter, and heart failure. The drug was toxic in higher doses.
Inaprovaline : A synaptic stimulant and cardiostimulant that fortified the cell membranes and could be used as a preventative measure or in response to various physical illnesses and states.
Lectrazine : A drug that could be used to stabilise the cardiovascular system in the event of shock or disruption in normal cardiac functions.
Metrazene : A drug that could be used to treat cardiac arrhythmias.
Quadroline : An emergency resuscitative drug that was used to treat cardiac arrhythmias.
Stenophyl : A drug that could be used to treat anaphylactic shock.
Neurological
Alkysine : A drug that was used to reduce the damage caused to neurological tissue following the event of a catastrophic injury.
Cortical Analeptic : A type of drug administered via hypospray to reinvigorate tissue within the cerebral and motor cortex following disruptions to the neural functions.
Synaptizine : A drug used to treat neuroleptic shock.
Theragen Derivative : A compound that could be used to deaden nerve inputs into the brain, resulting in a calming effect on the patient and a reduction in emotions such as anxiety, stress and aggression.
Trianoline : A medicine used to help patients with percussive injuries in small doses; 0.4ccs was sufficient for a concussion.
Vertazine : A drug used for to aid recovery from severe dizziness and vertigo.
Arithrazine : A medication used in extreme cases of theta radiation poisoning. It could also serve in the form of an inoculation. A medical officer was required to monitor a patient receiving arithrazine during treatment according to Starfleet medical protocol.
Analeptic Compound : A compound used to counter the detrimental effects of certain types of radiation, including theta radiation.
Hyronalin : A drug used to counter the effects of radiation poisoning. These effects can be enhanced when combined with lectrazine.
Recreational and Narcotic
Alcohol : A chemical that acted as a psychoactive drug with intoxicating effects when consumed, known to be addictive and to possibly result in poisoning when consumed in high quantities. It could also be used as a disinfectant and as an antiseptic gel.
Caffeine : A stimulant consumed in a variety of foods and beverages. If consumed regularly, it could become addictive, along with causing side effects such as insomnia, gastrointestinal distress and hypertension.
Felicium : An addictive narcotic that granted the user a euphoric sensation with both pain-relieving and sedative side effects. Serious withdrawal symptoms tended to occur within 72 hours.
Impedrezene : A narcotic that slowed down higher brain functions and affected motor function. Extreme headaches were commonly found when the effects wore off.
Ketracel-White : An addictive narcotic given to Jem’Hadar soldiers by the Dominion to provide an essential enzyme, as well as all the nutrients they required to survive.
Synthehol : A chemical that replicates the properties of alcohol, without the effects of intoxication, addiction, or poisoning.
Triglobulin : A drug used by some species as an aphrodisiac, though also had an application to aid in the facilitation of vaccinations and medicines.
Respiratory
Cortolin : A resuscitative drug that was primarily used in reviving patients who had stopped breathing.
Dexalin : A drug used in the treatment of oxygen deprivation.
Pulmozine : A drug used to treat oxygen deprivation and stimulate breathing.
Trioxin : A drug used in the treatment of respiratory injuries, though only appropriate in emergency situations as a stop-gap measure.
Resuscitative
Cortolin : A resuscitative drug that was helpful in reviving patients who had stopped breathing.
Leporazine : A resuscitative drug that had minimal chance of causing negative effects, but could not be administered to a patient with low blood pressure.
Morathial : A drug similar to leporazine, a series of which were almost as effective at resuscitating patients as the aforementioned drug, without the risks to the patient's blood pressure.
Netinaline : A stimulant that could be used to resuscitate a patient.
Ambizine : An injectable drug that was used as a fast-acting sedative.
Anesthizine : A fast-acting anesthetic typically deployed as a gas. It was considered to be one of the best by the Federation .
Dylamadon : A sedative that could be used to simulate death in an individual.
Improvoline : A standard sedative that could be used in smaller doses, such as 5ccs, to calm and pacify a patient. Higher doses would be able to keep a patient sedated for longer periods of time.
Kayolane : A standard sedative that caused unconsciousness for several hours.
Melorazine : A standard sedative.
Merfadon : A less effective sedative that could be rendered inert depending on the diet of the patient.
Tetrovaline : A medical drug that renders a person unconscious, but also lowers immune response.
ADTH : A stimulant which could be dispersed in a gaseous form through the life support system of a typical Federation Starship.
Animazine Derivative : A stimulant that could be used to awaken someone from sleep, or keep them conscious for longer durations than naturally advised.
Cortropine : A stimulant found in standard-issue medkits which could stimulate the recipient to overcome symptoms of weakness or fatigue.
Dalaphaline : A systemic stimulant that can strengthen individuals after neurological.
Formazine : A stimulant that could be used to promote alertness and reduce fatigue, however in higher doses could cause restlessness and irritability.
Hyperzine : A standard stimulant that could be used to counter seizures.
Masiform D : A powerful stimulant that could be used to counteract the effects of poisoning. It had a side effect of an upset stomach in Vulcans .
Polyadrenaline : A synthetic version of adrenaline that could be used as a stimulant which could aid the revival of a patient who had died or was near death.
Tricordrazine : A highly potent stimulant that could be used both to resuscitate and as an anti-seizure medication. However, doses higher than 10ccs were risky.
Benzocyatizine : A medication used to treat low isoboramine levels in Trill , which regulated the connection between symbiont and host.
Cervaline : A drug used to limit rejection of transplanted organs or tissue.
Dylovene : An antitoxin carried as standard in Starfleet medkits
Mirazine : A drug used to reduce the time necessary for decompression when boarding and leaving starships.
Priaxate : A drug used to lessen the symptoms of plague.
Stokaline : A multivitamin drug administered via injection.
Tesokine : A drug used to facilitate cross-species surrogacy.
Disclaimer Notice
- Starfleet Medical Emblem used with permission of Gazomg Art - granted Nov 24, 2016
- List of medical instruments used with permission of USS Wolff CO - granted Jan 30, 2017
- List of drugs and medications obtained using information from the public domain at Memory Alpha - obtained Oct 5, 2018
- Information Source: Star Trek: Adventures, Science Division Rulebook
- Departments
- More to Explore
- Series & Movies
Published Nov 5, 2019
How Modern Surgical Tech is Approaching Star Trek's Future
The PIRL Scalpel may not be the final frontier in surgery, but it's pretty close.

StarTrek.com
In every iteration of Star Trek , from The Original Series to Discovery , there are always a few scenes where a medical officer whips out a tricorder or dermal regenerator, waves it over an injured crew member, and fixes up their injuries without leaving a trace.
This sort of medical care might seem like something that could only happen in the distant future — if it could happen at all — but new developments in medical laser technology by a team led by University of Toronto professor Dr. R.J. Dwayne Miller are moving some of what we see on screen away from science fiction and towards science fact.
“I think the thing that’s interesting about Star Trek is that the writers — and all sci-fi writers — let their imaginations go wild and ask ‘wouldn’t it be great if…?’” said Dr. Miller, who grew up watching the show. “And science, eventually, by some circuitous route, sometimes does find things that look very similar to what they imagined.”

When Theodore Maiman successfully fired the first laser in 1960, just six years before Star Trek first aired, people almost immediately recognized its potential uses as a surgical tool. In theory, by focusing energy towards a specific place, lasers should allow a surgeon to make precise cuts even in hard-to-reach areas of the body. But there were significant downsides to this approach.
“The problem isn’t getting energy down to the dimension of a single cell,” Dr. Miller explained. “The problem is confining energy. You put the energy in, and what would happen is that it would thermally diffuse. The temperature of the adjacent tissue would get above the combustion point, and you would get horrific burning.”
On top of that, there was the problem of cavitation, also known as 'bubble collapse' — lasers cause specific areas of tissue to undergo phase transitions, turning them from a solid to a liquid to a gas. Dangerous bubbles can form and spread during this process.
“Think about boiling a pot of water,” Dr. Miller said. “Next time you do this, look at the bottom of the pot. You’re going to see there’s little nucleation sites everywhere — bubbles grow and grow and then they violently collapse. That’s what happened when you used lasers for surgery … [I’ve seen surgeries where] cavitation shockwaves led to collateral damage away from the cuts.”
Since the 1980s, Dr. Miller has been trying to figure out a way around these problems. Armed with new discoveries that his lab made over more than a decade about the atomic and molecular structure of water, he posed the question: what would happen if you had a laser that fired extremely high-energy pulses, cutting so quickly and for such a brief time that bubbles wouldn’t form, and the surrounding tissue wouldn’t burn?’
So, he and his team built that laser, called the Picosecond InfraRed (PIRL) scalpel.
“The very first time we used it was just on skin tissue,” he said. “[For comparison] when you do surgery with a conventional laser, you see smoke, it looks horrible, you can see massive damage where you’re cutting. When you look at our laser, it’s just melting away at the tissue. You don’t see any smoke. It looks like you’re breathing into cold air.”
The PIRL scalpel also makes it possible to do scar-free surgery — if handled properly, once the cuts are healed, they are totally invisible.

ResearchGate
“When you would watch Star Trek , they would seemingly solve different things and instantly heal injuries,” Dr. Miller said. “Well certainly, now we can cut at that ultimate limit [of precision], and the healing, if you do bonding with bio-compatible glues, would literally look like the Star Trek thing. Actual scar-free healing takes time. But if you hold it and glue it, it would look — from a visual perspective — like it healed instantly.”
Surprisingly, scent was one of the more interesting developments to come out of the invention of this new tool. Dr. Miller’s laser scalpel allows doctors to actually smell the difference between different types of tissue as they cut, whereas with previous tools you could only smell the burning. This could have major implications for how surgeons work in the future, warning them when they’ve moved too far off track and even signaling the difference between healthy and diseased tissue.
“It turns out that the water is perfect at ejecting entire protein complexes into the gas phase, and we have a complete signature of what is being cut,” Dr. Miller explained. “Now, you’re talking about turning any surgeon into a super-surgeon, because you’re basically getting a barcode for what tissue is being cut.”
While the PIRL scalpel might well make modern-day hospital operating rooms look and function a lot more like Sickbay on the Enterprise, Dr. Miller has no illusions about the glamor (or lack thereof) of the years of research that brought him and his team to this point. Still, he says, it has all been worth it.
“Science is not all ‘eureka’ moments and fun and games,” he said. “It can be frustrating. You have to have a deep-seated drive to solve a problem, and maybe you have to be a little bit nuts to do it. It’s competitive; it’s a contact sport. Peer review is rigorous, and you have to respect the process. Science takes a lot of hard work. It doesn’t work the way you always think – and thank goodness, because otherwise we’d already know the outcome. And the reward is in the end – you get to go to a very beautiful place where nobody else has been. We get to go where no one has gone before.”
And Dr. Miller had a few words of encouragement for scientists who are currently embarking on their own journeys of discovery.
“You never know – by definition – where it’s going to go,” he said. “But, whatever the voyage, it’s going to be beautiful.”
Julia Peterson (she/her) is a queer Jewish journalist currently based in Regina, Saskatchewan. She also writes for INK Magazine, The Carillon, and Reading in Translation, and would give just about anything to have a pet tribble. Find her on Twitter @hark_a_julia.
Get Updates By Email
Continuing Mission
A Fan Site for the Star Trek Adventures RPG by Modiphius

REPLICATOR RESOURCES: MEDICAL REFERENCE GUIDE

Gotta’ love the fans of Star Trek Adventures, constantly creating new guides, tools, and resources to enhance the universe’s best RPG. Today’s gift comes from Jason Marden.
Medicine is an inherently complex field, and Starfleet medical officers have access to a wealth of medical equipment. Some of it is portable and can be taken along on away team missions, while much of it can only be used in a hospital or sickbay. The Star Trek Adventures Starfleet Medical Reference Guide describes some of the more important and common medical devices that have not previously been described, all granting a particular Advantage or rule with its use. Common equipment that is part of a medkit, which has no Opportunity Cost, may not have a unique benefit.

Star Trek Adventures – Medical Reference Guide
PDF VERSION: STA -MEDICAL REFERENCE GUIDE
When asked to brag about himself, contributor Jason Marden said, “Hi, I’m Jase but you might know me as Hairy Gamer Jase. I’m a proper nerd covering wargaming, board games, LARPing, hobbying, 3d printing and of course RPGs. I’ve been a Trekkie since forever and have been playing Star Trek Adventures since the playtest. I have a long-running campaign set in 2372 aboard the USS Exeter following ten, yes ten characters as they embark upon a Five Year Deep Space Exploration mission into the Shackleton Expanse.”
We at Continuing Mission love it when superfans make such valuable contributions to the game. If you have something you would like to share, reach out to us. You can hit me up personally at michaeldismuke1 at gmail dot com.
Share this:
Wow! Amazing work! But… do we need to ask permission to download it? When I clicked on it, it was “read only”…
Oh. Let me check if I can grant permission for that.
Added a downloadable PDF for ya’!
Leave a Reply Cancel reply
This site uses Akismet to reduce spam. Learn how your comment data is processed .
Discover more from Continuing Mission
Subscribe now to keep reading and get access to the full archive.
Type your email…
Continue reading
Being a CMO or MO is a very challenging position on a ship. Considering Medical personnel are not always on the bridge, we are more easily over looked than other positions. In the information that follows, you will find resources that will give you ideas to help keep yourself busy if and when the SM is not able to. The information also details the duties for both the CMO and MO. It lists diseases, medicines, medical treatments, and medical equipment. It gives you a template to help design a species for an arc if your SM has developed one. There is a plethora of information we hope you find most useful as you serve in ST:EQ as a part of the Medical Department.
Chief Medical Officer's Duties
The CMO's duties fall under two main categories. He or she has medical duties as well as Administrative duties.
Medical Duties
Medical problems, prevention i.e. physicals.
- Upon new assignment: Each person should receive a complete physical on two different occasions. Everyone is supposed to receive a yearly physical. Also, upon assignment to a new starship or Starbase, everyone should receive a baseline physical. During this physical four readings (heart rate, blood pressure, respirations, and temperature) and ten scans (Cranial scan, Brainwave scan by hyper-encephalogram, Bronchial scan, Gastrointestinal scan, Muscular scan by resonance tissue scanner, bone scan, cardiovascular scan, blood scan, lymphatic scan, reproductive scan) should be performed.
- Although most people don't do these regularly. Partial physicals are supposed to be done when a crewmember returns from an Away Team. Four readings (heart rate, blood pressure, respirations and temperature) and two scans (Brainwave scan by hyper-encephalogram and blood scan) should be done for this physical.
If as a Chief Medical Officer you aren't able to prevent diseases or injuries, your secondary purpose is the diagnosis of illnesses and diseases. You can find a list of these in Appendix A . You can also find a list of different Starfleet scans, tests, and screenings in Appendix B .
Once as a CMO you've diagnosed an illness or injury, there are two ways that treatments can be rendered, technological treatments and pharmaceutical treatments. Technological treatments are found in Appendix C . Pharmaceutical treatments are found in Appendix D . Appendix E lists medical equipment you can use to accomplish your treatments.
Away Team Duty
Depending on the mission, often a medical officer is sent along on the away team. Their main job of course is to see to any injuries that may occur to any member or the away team or any other medical emergencies.
Research : In the context of Mission Orders being sent with the purpose of research, medical often supports science, or replaces them if there is no science officer on the AT. Where science is scanning for everything under the sun, medical's main concern is anything that has to do with the biological. Biological includes plants, animals, insects, birds, fish, bacteria, microbes, anything defined as living.
Medical Assistance : There are times when a ship will be sent out to help another ship who is in the midst of a ship wide medical emergency. Medical on the ship will lend assistance to the ship on which the emergency is located.
Relief Aid : There are other times when planets may be in the midst of planet-wide or even a localized epidemic. Starships may be called in to assist or bring medical aid. In cases like this Medical may be called upon to research, diagnose, and treat the medical ailment. Often times discussing facts with your SM will be of great value. He or she will usually provide some information upon which you can go in hopes of solving the medical situation.
Medical Briefings
A medical brief is often collaboration between the CMO and the SM. They are not written up as often as science briefs, but in cases where biological or medical are the underlining theme, they can add to the storyline. They also give the other players references to use so that everyone is using the same language and has the same basic knowledge of what is going on.
Often the SM will give the CMO a free hand with a medical situation, giving them the key points that need to be included or in some cases, left out. Unless the medical personal is fairly certain of their SM and what they expect, the Medical Brief should be sent to the SM for approval before sending out. The MB is usually attached as a supplemental to ones log for that week in the NG unless otherwise suggested by the captain, in which case it can be attached to the ships Mission Brief.
A distinction needs to be made between a Medical Brief that is sent out and one that is done during a mission during a meeting. If one knows they will be presenting data during a meeting they should pester the SM before hand for any information they might need. If possible, have it typed up and prepared to give before hand to save mission time. Otherwise, those mission briefs are often a gathering of facts that have already been given and you are now presenting it combined and in a medical genre to send out with your log.
Medical Drills
In planning medical drills you will need to take several things into consideration.
- Decide if the drill is meant as a character development tool (OOM) or if it is to interact with different ship departments. (In mission)
- Ask your SM's and Captain's permission (if you want to do this in mission).
- Decide on a scenario that will be used to test the ship's medical readiness.
- Consider recruiting NPC's or crew to assist in the drills.
Supervising
During in mission drills, you may find yourself needing to direct certain characters' actions a specific way. Feel free to give them information that will motivate them to make moves that you need.
Sometimes Mission Orders will state that you will be doing medical research on a particular species of plants or beings. It is strongly suggested, that until you are absolutely positive that what you are studying is safe, that you keep it in some kind of containment field. When working with this type of mission, make sure you ask as many question.
Other times, research can be done during the course of a routine mission that has nothing to do with medical. If you find yourself in one of those situations in which medical is either underutilized or not utilized at all devise a scenario that gives your character some medical research to do.
Administrative Duties
Out of character.
It is suggested that if you have a created staff for all areas and shifts, that you might create a short profile for them for the crew to use in their logs. This works well when the crew needs or wants a doctor and either doesn't want to bother the CMO or the CMO is not readily available for OOM's or log permissions.
In Character
Assigning Medical Staff's duties : The CMO is responsible for assigning the medical staff's duties. Take a look at the different units that are on your ship and assign NPC's to cover those aspects. You can do this for a log idea or in character during a mission slot.
Setting Medical Staff's schedules : The CMO is responsible for setting the medical staff's schedules. Again, create a list of your medical NPC's, their ranks and positions (MO, Med Tech, Nurse, etc) and schedule them for certain shifts. Again this can be done in a log or in the context of a mission.
Searching for or replacing medical staff : This is an area in which you can do a lot of character development. You can ⤽interview� people for the position, spend time talking to the NPC's superiors, etc.
Supervising Medical Staff : This can fall under so many categories. This can be done during medical emergencies or it can be done as part of a routine happenings. Even the simplest of tasks, that as a CMO, you supervise can become great log or interaction ideas.
Medical Officer's Duties
- Upon new assignment : Each person should receive a complete physical on two different occasions. Everyone is supposed to receive a yearly physical. Also, upon assignment to a new starship or Starbase, everyone should receive a baseline physical. During this physical four readings (heart rate, blood pressure, respirations, and temperature) and ten scans (Cranial scan, Brainwave scan by hyper-encephalogram, Bronchial scan, Gastrointestinal scan, Muscular scan by resonance tissue scanner, bone scan, cardiovascular scan, blood scan, lymphatic scan, reproductive scan) should be performed.
If as a Medical Officer you aren't able to prevent diseases or injuries, your secondary purpose is the diagnosis of illnesses and diseases. You can find a list of these in Appendix A . You can also find a list of different Starfleet scans, tests, and screenings in Appendix B .
Once as a MO you've diagnosed an illness or injury, there are two ways that treatments can be rendered, technological treatments and pharmaceutical treatments. Technological treatments are found in Appendix C . Pharmaceutical treatments are found in Appendix D . Appendix E lists medical equipment you can use to accomplish your treatments.
Medical Assistance : There are times when a ship will be sent out to help another ship that is in the midst of a ship wide medical emergency. Medical on the ship will lend assistance to the ship on which the emergency is located.
Assigned Duties
The MO should carry out orders as assigned to him or her by the CMO. When the CMO is not present, whether they are on an Away mission, or unable to make a mission, the MO steps in and basically covers for the CMO duties.
Appendix A: Star Trek Illnesses
Appendix b: star trek medical scans, tests, and screenings, appendix c: star trek medical procedures, appendix d: star trek medicines, appendix e: medical equipment, appendix f: ship's medical facilities, main sickbay.
These facilities provide the medical staff with an impressive complement of tools with which to handle an extraordinary range of medical problems for both known and presently unknown species. Capabilities include a fully equipped medical laboratory with advanced bio-assay and life form analysis hardware. Also available are nanotherapy, genetic sequence, and viro-therapeutic equipment. Medical lab capabilities can be bolstered by employing the lab services of one or more shipboard science department.
Surgical Suites
A key element to the medical intensive-care unit is the biobed sensor and support unit. This orthopedically designed hospital bed incorporates a basic array of bio-function sensors that can be tied into a variety or remote medical instruments including the medical tricorder. Also incorporated are a number of medical gas and fluid connect points for various devices, including the surgical support frame.
A vital tool in nearly all surgical procedures is the surgical support frame (SSF), or 'clamshell' as it is sometimes called. The SSF not only maintains a sterile environment for most surgical procedures, but also incorporates several vital diagnostic and life support tools. These include a battery of bio-function sensors, supplementing those provided by the biobed and by the overhead medical equipment array. The SSF is capable of automated administration of intravenous medication as well as cardiovascular support and emergency defibrillation. A variety of surgical support frame types are available for different procedures, as well as for different life form types. Most biobed units are designed to accept surgical support frame.
Surgical procedures and other intensive care procedures are accomplished at the primary biobed, located at the center of each sickbay ward or surgical suite. Above this biobed is an overhead cluster of diagnostic bio-function sensors. This array also incorporates a low-level force field generator that can be used to reduce the chance of potentially harmful microorganisms entering or leaving the biobed area. Not that this force field is of relatively limited utility and is not adequate to maintain a totally sterile environment sufficient for surgical procedures or to satisfy biohazard protocols.
Most medical treatments occur in the ICU (Intensive Care Unit), which has several biobeds, which can perform all the functions of a medical tricorders MP unit.
Null-gravity Therapy Ward
When a person's injuries are severe to the point they are not able to bear weight on a lower extremity or they have extreme pain during motion, the Null-grav ward is used to remove any downward pull on the limb from gravity.
The purpose of the morgue is two-fold. It is to store bodies of deceased crewmembers and family who resided shipside or station-side. The morgue is also designed to handle autopsies not only of crewmembers and family, but also of alien physiologies.
Biohazard Unit
The biohazard unit is designed to handle a situation where someone has been exposed to a bio-hazardous material. This unit allows isolation from the rest of the ship air and water supply as well as for decontamination of the pathogen or other bio-hazardous material.
Isolation Unit
The isolation unit is designed for the isolation of a patient who could contaminate the ships population through direct contact, indirect contact, or airborne means. This unit keeps the patient completely isolated from the ships population. Even the air used in this unit is filtered by a different system and is not spread throughout the ship.
Dental Care Office
Dentistry also falls under the jurisdiction of the Medical Department. The Dental care office is expressly for that, dentistry. A tech specialized in dentistry will care for the teeth of those onboard ship in this office.
The nursery is where babies are kept for at least the first few hours of their lives while their mothers recover from childbirth. Also babies who have had troubles during the birth or babies who have special needs are kept here for treatment.
The laboratory onboard a starship or station is equipped to handle most work ups that need to be done whether it be culturing an unknown bacteria or running tests on blood that can be done on a tricorder. Almost anything that can't be done on a tricorder or a biobed sensor panel can be done in the laboratory.
Physical Therapy Unit
Its name states its basic purpose. This unit is designed for and houses equipment used in physical therapy. If and when a crewmember is injured to an extent that even surgery cannot fully repair, physical therapy is done in this unit.
Radiation Therapy Unit
When a crewmember has been exposed to near fatal levels of radiation for a short time or has been exposed to harmful levels of radiation over a long period, the treatments found in this unit can help save lives.
Critical Care Unit
This is a unit where critically ill patients can receive more comprehensive treatment. Many times when a doctor has exhausted all of his or her treatment options for a terminally ill patient, the patient will spend the rest of onboard ship time here.
Aide Stations
Aide stations are very similar to a mini Sickbay. They can do many things that main sickbay can do but they have no other lab facilities or specialized treatment facilities attached. If a person with serious injuries is brought to the aide station, stabilizing medical treatment can be given and then the patient will be sent to main sickbay where they can obtain more comprehensive treatment.
Extra Emergency Medical Facilities
In large-scale medical emergency situation, all shuttle bays can be converted to medium- and intensive care hospital facilities using quick-deploy emergency hospital modules. Additionally, lesser numbers of overflow patients can be handled by conversion of guest quarters to medical intensive-care units.
Appendix G: Description and breakdown of Medical Personnel by shifts
Station information.
According to DS9 tech manual on a station the medical department in comprised of 10 staff physicians, 20 nurses as well as med techs. Each shift was comprised of one doctor, two nurses and two med techs. The rest of the staff are distributed between the laboratories and other research suites and are rotated to the infirmary in three shifts per twenty-six hour day. An overlap of some ten minutes allows the shifts to exchange updates during changeover. Research laboratory personnel not directly assigned to the infirmary rotation number anywhere between fifteen and twenty-five, are scientists and techs that are working on projects.
Ship Information
A good example of the breakdown of medical personnel for ships would be along the following lines. Alpha shift would be comprised of the CMO, MO, one nurse, and two med techs. Beta shift would be comprised of an MO, one nurse, and one tech. Gamma shift would have an MO, one nurse, and one med tech.
Appendix H: Creating a new race for an arc
There will be situations where the SM will want to introduce a new race for an arc. Many times they will feed you pertinent information on a race and they will expect you to fill in the blanks in the information they gave you. The following information will give you a template you can use in allowing you to develop all aspects of a new species.
- Officer's Manual
Science-Based Medicine
Exploring issues and controversies in the relationship between science and medicine
Medicine past, present, and future: Star Trek versus Dr. Kildare and The Knick
I love the new Cinemax series The Knick , which is set in 1900 and portrays a brilliant maverick surgeon named Dr. John Thackery on the cutting edge of medicine at the time. I also love Star Trek ‘s Dr. “Bones” McCoy and have recently come to like the old radio show featuring Dr. Kildare. Looking at how the three shows portray medicine in their respective times led me to speculate on how much medicine in its time really is or isn’t barbaric, as McCoy would put it.

One aspect of all the Trek shows that always interested me was its portrayal of medicine in the 23rd and 24th centuries . After all, what doctor wouldn’t like to have a device like the tricorder that he could wave over the patient and come up with an instant diagnosis and course of treatment? Who knew, of course, that nearly 50 years after the first Trek episode first aired, we would have technology that makes the communicators on the original series (TOS, for those Trek non-fans) look primitive and large by comparison and that we’d be well on the way to developing devices that can do some of what tricorders did on the show. Throughout all the shows and movies, the medical technology of a few hundred years in the future is portrayed as vastly superior to what we have now, with 20th century medicine at times denigrated by “Bones” McCoy and other Star Fleet medical personnel as barbaric quackery.
A confluence of events and media led me to want to explore a couple of questions. First, which procedures that we consider state-of-the-art science-based medicine will be considered “barbaric” 50 or 100 years from now? Second, is the contempt expressed for the medicine of the past (e.g., by “Bones” McCoy) justified? These are questions that I’ll explore a bit with the help of the Star Trek universe, a recent new cable television drama series, and a couple of articles that appeared on medical sites as a result of the premier of that series.
Star Trek : 23rd century medicine vs. 20th century medicine
Perhaps the most amusing example of McCoy’s contempt for the “primitive” medicine of the 20th century occurs in the 1986 movie Star Trek IV: The Voyage Home . (I found it particularly amusing because I was a third year medical student when the movie came out.) For the purposes of this post, you don’t need to know the plot, other than that it involves the crew of the Enterprise time traveling to San Francisco in the year 1986 to obtain something from the past that would save the Earth of the year 2286. During their mission one of the crew, Chekov, is seriously injured fleeing from the military, captured, and as a result taken to Mercy Hospital for emergency surgery. When Dr. McCoy learns of this, he begs Captain Kirk not to leave Chekov in the hands of 20th century medicine. So Kirk and McCoy disguise themselves as doctors and infiltrate the 20th century hospital where Chekov is about to undergo emergency surgery in order to rescue him. It is during this part of the movie that this hilarious exchange occurs:
For those of you who can’t play the YouTube video, here’s a transcript that shows you what I mean. First, “Bones” encounters an old woman on a gurney in the hallway and asks her a question:
McCoy: What’s the matter with you? Patient: Kidney… dialysis. McCoy: Dialysis?! What is this? The Dark Ages? Here! You swallow that and if you have any more problems, just call me!
Later, as the crew is escaping, McCoy encounters the woman again, who’s telling everybody that McCoy had given her some pills and she grew a new kidney .

In another scene, Kirk and crew are in an elevator with some interns, and McCoy overhears the following conversation, not being able to stop himself from butting in:
1st Intern: So, Weintraub says radical chemotherapy or she’s gonna croak. Just like that… 2nd Intern: And Gottlieb? 1st Intern: Well, what’d you expect? All he talked about was image therapy. I thought they were going to punch each other. McCoy [Muttering and shaking his head]: Unbelievable… 1st Intern [Turning to McCoy, having heard his muttering]: You…have a different view, Doctor? McCoy: Sounds more like the goddamned Spanish Inquisition! Kirk [Turning to the interns and shrugging shoulders]: Bad day…
Later, Kirk and McCoy kick a neurosurgeon about to operate on Chekov to drain what sounds like an epidural hematoma out of his operating room at phaser-point, and McCoy proceeds to save Chekov’s life with his 23rd century technology.

The Knick : What a difference 114 years makes!
Although I subscribe to HBO, I don’t subscribe to Cinemax. Consequently, I was only able to view the first episode of The Knick using On Demand, and have since only seen the first three episodes because HBO happened to show them all in a block about a week after the third episode aired. I haven’t seen episodes four or five yet, although I’m seriously tempted to subscribe to Cinemax for the remainder of the season just to see the show and then to drop it after the show’s run ends. However, the episodes I’ve seen are enough to pique the interest of any surgeon interested in the history of surgery. Producer Steven Soderbergh likes to brag about the measures his team has taken to assure historical accuracy with respect to the medicine practiced and the surgical procedures portrayed, particularly how extensively his show has used the Burns Archive, a trove of more than a million historic photographs (a few of which are digitized and displayed here , unfortunately without much in the way of text or captions to tell the viewer what they are), to recreate the look of medicine in the early 20th century.
Of course, it being a fictional show, there are things that The Knick takes some creative license with , such that I wondered about them immediately. For instance, body snatching to supply hospitals with medical cadavers and fights between ambulance drivers over who gets to pick up patients were apparently not as prevalent as The Knick portrays, given that New York was one of the first states to pass “ anatomical acts ” in the mid-19th century to discourage trade in bodies and body snatching. By 1900, such activities would be a risky, at best, crime not likely to be particularly profitable. On the other hand, given the level of endemic corruption in New York in 1900, characters like corrupt Health Inspector Jacob Speight who takes kickbacks to refer patients he finds with reportable infectious diseases for which the city mandates treatment to the Knick and the equally corrupt hospital administrator who works with him are not implausible.
One thing I noticed in the very first operating room scene (and in all the operating room scenes in the episodes I’ve seen thus far), surgeons are depicted operating bare-handed. Instead of scrubbing up and using rubber gloves, as surgeons have done for many decades now, they dipped their hands into antiseptic solution right before the start of surgery. It turns out that the great surgical pioneer upon whom Dr. Thackery is loosely modeled , Dr. William Stewart Halsted had pioneered the use of rubber gloves in 1889 or 1890 because his scrub nurse (with whom he later fell in love and who ultimately became his wife) had begun to develop severe contact dermatitis as a result of the nasty chemicals (mercuric chloride and phenol) used to disinfect the hands of the operating staff at the time. Rather than have her reassigned, Halsted requested the Goodyear Rubber Company, as an experiment, to make “two pair of thin rubber gloves with gauntlets.” At first, only assistants used them, but within a couple of years, the surgeons at Johns Hopkins, where Halsted practiced, were using them. So it seems a bit of creative license that the surgeons at the Knick would still be operating bare handed. On the other hand, it’s not too beyond the pale that some surgeons might still be operating bare handed in 1900, given that it wasn’t until 1899 when Halsted’s protégé Dr. Joseph Bloodgood (what an awesome name for a surgeon!) published a report of 450 hernia operations using gloves, observing that the infection rate fell by nearly 100%. Bloodgood’s report led Halsted to take himself to task, asking “Why was I so blind not to have perceived the necessity for wearing them [rubber gloves] all the time?”
Think of it: A man with one of the most brilliant minds in the entire history of surgery responsible for so many surgical innovations, from emergency blood transfusions, to cancer surgery, to something as mundane as a bedside chart to track a patient’s vital signs and the use of surgical gloves operating room, a man who first laid down surgical principles still taught to all surgeons today, such as a completely sterile surgical field, hemostasis, gentle handling of tissue, careful anatomic dissection, and exact approximation of tissues, and Halsted couldn’t immediately figure out that wearing sterile rubber gloves instead of dipping one’s hand in caustic chemicals to disinfect them was a superior means of preventing surgical infection!
Other examples, although perhaps anachronistic, are found in the fictional world of The Knick . For example, the very first OR scene in the very first episode portrays the attempt by Dr. J.M. Christiansen and Dr. Thackery to perform a Caesarian section on a woman with placenta previa, after having failed at this procedure eleven times before. They fail again, with the mother and baby both dying. As a surgeon, I found this scene particularly disturbing and effective. As I watched the impressively realistic pools of blood form, overwhelming the ability of the pedal-driven suction to clear them, the surgeons frantically working, and the nurse reporting a faster and faster pulse (and ultimately no pulse), all as dozens of doctors and trainees observe the procedure, I couldn’t help but wonder how surgeons could actually save anyone in such an environment.
The same question came up later in the same episode, when a man with a bowel perforation had his injury repaired primarily. The surgeon who did the repair was taken to task by Thackery on rounds for not resecting. Later, the patient develops intra-abdominal sepsis, requiring Thackery to operate on him using an instrument he had constructed himself to resect the nonviable bowel and sew it back together. While I admit that this part made me wonder (bowel anastomoses were pretty standard procedures by 1900; so I’m not sure why this would have been so revolutionary), I still had to marvel how any surgeon could expect any patient with a bowel resection to survive intra-abdominal sepsis after a bowel perforation with no antibiotics as adjunctive care for the drainage and resection.
More examples included a man with an aortic aneurysm, for whom the treatment would be a galvanic procedure (using electricity to induce thrombosis of the aneurysm), an attempt to reconstruct a woman’s nose lost to syphilis using a tissue flap from the arm that necessitated the arm to be attached to the nose for several weeks to provide a blood supply (a technique still in use today for some reconstructive procedures), and the portrayal of Dr. Thackery anesthetizing a patient using a cocaine epidural. A lot of these weren’t exactly 1900 medicine, although they were generally from within a few decades. Dramatic license again. The point, however, is that medicine always operates within the context of the existing scientific and clinical knowledge of the time. Of course, The Knick is a vision of what medicine was like in 1900 imagined by a man of 2014. However, it’s also informative to look at medicine as portrayed in the media contemporaneously, as we will see. To do that, I leap from the world of The Knick to 50 years in its future.

Dr. Kildare, or I’d rather have a bottle in front of me than a frontal lobotomy
Over the last few years I’ve become a bit of a fan of old time radio , having discovered Radio Classics on Sirius XM Radio. In particular, I discovered The Story of Dr. Kildare . This particular radio show stared Lew Ayres as Dr. Kildare and Lionel Barrymore as the irascible Dr. Leonard Gillespie (the latter of whom was actually hilarious, by the way). It’s an episode of this show that demonstrates perhaps the clearest example of a standard of care that turned out to be disastrously wrong.
I sometimes listen to Dr. Kildare not so much for the stories themselves, but because of what a time capsule the show represents when it comes to how medicine is practiced. Most of the radio episodes I listen to tend to be from the early 1950s. One episode remains stuck in my mind, an episode that originally aired February 1, 1950 entitled “ Angela and Steven Kester “. The episode begins with Dr. Kildare showing up in his office on a typical morning to cover a long shift on duty. He’s greeted with a phone call from an old friend named Angela Kester. Kester used to be a famous concert pianist, but in this phone call she frantically begs Dr. Kildare to come right away to her apartment because she’s convinced that her husband is planning to kill her. Dr. Kildare protests that he’s on duty and can’t easily leave the hospital, but she’s so upset that he tells her he’ll be right over. On his way out the door Dr. Kildare runs into Mrs. Kester’s husband Steven, who has come to visit him. Kester tells him that he’s very worried about his wife, who, according to him, appears to be exhibiting obsessive behaviors, playing the same piece over and over again, sometimes practicing 16 hours a day. Apparently, five years prior at a concert at Carnegie Hall, she suffered a breakdown and couldn’t perform in front of an audience after that. Kildare informs Kester that his wife had just told him that she thought Kester was trying to kill her. Kester, not surprisingly, is horrified, and the two of them rush over to the Kesters’ apartment, where they encounter Mrs. Kester feverishly playing and yelling that her hands are being controlled by the music.
Later, we learn that Mrs. Kester’s father had been a “second rate” pianist who had wanted his daughter to succeed where he failed. Recognizing Angela’s talent at a young age, he spent lots of money on lessons for her and pushed her harder than any father should push his child, taking pains to make sure that Angela was constantly reminded of just how much he had sacrificed for her. We also learn that she had undergone insulin shock therapy, a treatment in which large doses of insulin were administered to induce a hypoglycemic coma, a treatment that fell out of favor a few years after this particular episode aired because not only did it not work but it was very dangerous given that hypoglycemia can easily kill. We then learn that Angela Kester had undergone many cycles of electroconvulsive therapy , with little or no improvement. Much discussion occurs about how Angela couldn’t tolerate another course of ECT or insulin shock therapy.
Around this point, Angela tries to commit suicide by shooting herself in the chest, but fortunately for her all she did was to give herself a pneumothorax . Dr. Kildare operates and easily saves her life. Angela’s suicide attempt, however, leads Dr. Gillespie and Dr. Kildare each independently to delve into the medical literature looking for answers (one of the better aspects of this particular episode, as disturbing as the solution they both ultimately found was). The solution they come up with? They both decide that a prefrontal lobotomy is Angela’s only chance to be “cured” of her condition.
So, even though Dr. Kildare was a fictional surgeon, in this episode we see him diagnosing Angela with paranoid schizophrenia (which in all fairness was probably an accurate diagnosis), obsessive-compulsive disorder, and neuroses. In any case, not surprisingly, given the framing of the choice in such terms, the decision is made to go ahead with the operation, even though Dr. Kildare is not a neurosurgeon and appears not even to have performed this particular operation before. None of this stops Steven Kester from agreeing to the operation on behalf of his wife, and the operation proceeds. Dr. Kildare whips out the leucotome (a special instrument designed to use in performing prefrontal lobotomies) and does the operation, drilling a hole in Mrs. Kester’s skull and using the leucotome to cut the connections between the prefrontal cortex and the underlying structures. Naturally, Dr. Kildare’s surgical skill is copiously praised when he finishes the operation. After a few days of suspense, during which everyone wondered whether the lobotomy had been successful, Mr. Kester demands to see his wife, who is initially afraid of him, but then, after she recognizes him, declares that her “hands are free,” meaning that she didn’t feel the compulsion to play anymore. She is declared “cured.”
From the perspective of 2014, this episode is disturbing in any number of ways. First, there is the demonization of mental illness that shows through even a seemingly sympathetic script. Words like “lunatic” and “lunacy” were thrown about not by lay people but by Drs. Gillespie and Kildare themselves to describe Mrs. Kester’s mental illness. In some ways, the desperation is understandable. 64 years ago, there was little that could be done in such cases, and it is not entirely surprising that a sense of desperation led to the conclusion that desperate conditions call for desperate measures, such as insulin shock therapy (a dangerous therapy that didn’t work), ECT (which could work and is still occasionally used in the case of severe depression refractory to medication but was hugely overused then), and, of course, prefrontal lobotomy .
Interestingly, this particular episode of Dr. Kildare aired right at the height of the lobotomy craze (and, quite honestly, that’s what it is best described as, as is evident from Mo Costandi ‘s description of the rise and fall of the lobotomy ). It’s therefore no coincidence that this episode aired in 1950. No doubt the writers were doing what writers of medical series frequently do now: Feature a new medical or surgical treatment as the focus of drama.
Discovering this episode a few months ago simultaneously fascinated and appalled me. Like most TV and radio shows, Dr. Kildare is a time capsule both of the popular perception of how medicine was practiced during its time and of how medicine actually was practiced at the time. We had the young gun surgeon, highly skilled and compassionate, willing to take risks and push the boundaries paired with the old curmudgeon of a doctor who serves as his mentor and, despite his crankiness, is often revealed to have a heart of mushy gold. The show featured portrayals of medicine as practiced then, and, much like medical TV shows today, had medical advisors to guide the writers. In 1950, the prefrontal lobotomy, although admittedly controversial even then, was an accepted standard of care that we now view with horror. But how many others are there?
Is today’s standard of care tomorrow’s horror?
All of this brings us back to the central question of this post, which was mirrored when The Knick first premiered over six weeks ago, by Dr. Sanjay Gupta at MedPage Today , who asked the question Is Today’s Standard Care Tomorrow’s Horror ? To supply fodder for the article, six physicians were polled by e-mail with this question. The answers were rather interesting, although some of them were more about politics than actual science-based medicine. For instance, Cherie Binns, RN, answered the question this way:
Talk of limiting care for geriatric patients or the multiply handicapped child (especially at birth) and limiting access to resources for those with chronic health conditions that utilize a majority of services and healthcare dollars available are certainly, if they become standards of care, something that will be mocked, misunderstood, maligned in another generation.
She also laments how the Affordable Care Act allegedly prevents patients from seeing skilled health care providers. Whether that’s true or not, it’s not really an answer to the question, at least not as far as I’m concerned. Even though few people would be unsympathetic to this point of view, her response is really is more a matter of value judgments and resource allocation than it is a matter of the scientific standard of care.
Disappointingly, a lot of the responses were like that. Only one respondent, Dr. Murali Doraiswamy, was bluntly honest:
Ninety-nine percent of treatments today will be viewed as harmful or unethical in the future; for example, most psychiatric treatments given to children or most back surgeries.
Personally, I think Dr. Doraiswamy vastly overestimates what percentage of treatments will be considered harmful or unethical in the future, given the high percentage of treatments currently used that are evidence-based. For instance, there are many surgical conditions that can’t be fixed unless the anatomy is fixed. The operations aren’t going to go away; they’ll simply evolve to become less invasive, as they are doing now with the introduction of laparoscopic and robotic surgery and as the treatment of breast cancer has evolved from radical mastectomy to much less invasive procedures. Conditions like hypertension are still likely to require medication, as lifestyle changes, although they alleviate a lot of hypertension, won’t be enough for many people.
A more common example that came up was the use of “shotgun-style” or “one-size-fits-all” treatments, or, as one doctor put it, a “carpet bomb” approach to medicine. Of course, one doctor, Dr. John P. Higgins, has the opposite problem to go along with demonizing the past, namely a Pollyanna view of the future, in which he proclaims that “targeted and individualized therapy for a patient’s unique physiology will be used, with precision efficacy and near zero side effects.” There is little doubt that we will be able to target our treatments more and more effectively, but “near zero side effects”? Whatever Dr. Higgins is smoking, I’d want some if I could stand to inhale.
Let’s take an example that our good Dr. McCoy aimed his contempt at. It’s a treatment that’s commonly demonized not just by those who are—shall we say?—not completely down with the whole science-based medicine thing but even some physicians, chemotherapy. If you do a quick Google search, it doesn’t take long to find posts decrying chemotherapy for cancer as setting the standard for barbarism in the field and even as “ criminal .” Of course, there’s no doubt that chemotherapy is toxic and can be brutal (although it’s getting less so, thanks to better supportive care and more targeted therapies). However, as I’ve pointed out before, death from cancer can be far more toxic and brutal . When an ugly death is the consequence, chemotherapy’s risk-benefit ratio becomes more acceptable. Moreover, contrary to the claims of those who like to label chemotherapy as ineffective , chemotherapy, used appropriately, works . It’s also important to remember that most people who call modern treatments “barbaric” have an agenda that is not necessarily science-based.
Of course, there’s no doubt that chemotherapy has way more toxicity than we’d like, but to proclaim this issue a “ crisis ” is exaggerating. It’s more like a longstanding problem that will require research to overcome. Crisis or not, efforts are in full swing to find more targeted and less toxic therapies. It’s also true that individualized therapy, now more commonly referred to as “ precision medicine ”, will come to the fore. However, the process will not be as easy or fast as the hype promises . For every success , we will see failures . Moreover, we still don’t know what, exactly, “individualized” treatment will mean, even as quacks try to define it for themselves . Advancement in science-based medicine always occurs by fits and starts.
A rebuke to Dr. McCoy
As much as I love Dr. McCoy as a character, in that famous Star Trek IV hospital scene, he is dead wrong in his sneering contempt for medicine 300 years before his fictional time, just as I would be wrong to express the same sort of contempt for physicians from 1714 for believing diseases were a result of imbalances in the four humors, surgeons in 1900 who practiced without the benefit of antibiotics, or physicians in 1950 who were believing the case reports about frontal lobotomy. Physicians all practice according to the standard of the time, and that standard is based on the science as understood at the time. It is ridiculous to criticize physicians for not knowing something that hasn’t been discovered yet. In 2014 I hold in the palm of my hand a computer (my iPhone 5s) that is hundreds of times faster, drives nearly 2.5x more pixels, and holds thousands of times more data than the first computer I ever bought for myself, my clunky Mac LCII. Should I heap scorn on the computer engineers of a mere 22 years ago because computers then were so much less powerful than what we have now? Those engineers did the best they could with the technology they had.
I would also point out that science advances incrementally, building on what is known before, although there have been moments of rapid advance. It turns out that 1900 was a time of such advances in the field of surgery and medicine. Indeed, Dr. Thackery gives a remarkable eulogy in the very first episode for his friend who committed suicide, the very same Dr. J.M. Christiansen, who calmly walked into his office after his attempt at a C-section failed and the patient died, placed a sheet over the couch in his office, picked up a gun, laid himself on the couch, and shot himself in the head. This eulogy is particularly remarkable for its view of medical progress:
In particular, Thackery notes:
We now live in a time of endless possibility. More has been learned about the treatment of the human body in the last five years than was learned in the previous 500.
Many have said the similar things during the last few years, given the revolution in genomic medicine in which we currently find ourselves, and it’s true. We do live in a time of endless possibility, with amazing technology and science almost unimaginable by even the generation that preceded us. So, yes, I’d be shocked if some, or even a lot, of what we do right now as the standard of care is overturned even in the remainder of my career. I’ve already seen it just since I first entered medical school in the 1980s. It will continue, and that’s a good thing.
We are all products of the time in which we live, and we all have a tendency to view history through the lens of what is known now. To have a true understanding of the history of science, however, it’s important to try to put yourself in the shoes of physicians and scientists of long ago and take into account what they knew then and what tools they possessed. For example, the Halsted radical mastectomy is often decried as a “brutal” and “barbaric” operation. And so it seems to a surgeon of 2014. But remember: In the 1880s, when Halsted first conceived the operation, there was no chemotherapy, no radiation therapy, no adjuvant therapy of any kind. Breast cancers tended to present at an advanced stage. If a woman with breast cancer was to be saved, surgery alone was what would have to do it, without the highly effective help we surgeons now receive from our colleagues in medical and radiation oncology. In context, based on the understanding of cancer of the times, the operation made sense, and Halsted’s results were better than those of other surgeons. Similarly, today chemotherapy seems “brutal,” but it works. It’s the best that we have.
Going back to the fictional past of the Knick (and the real past), physicians in 1900 were just as clever, just as dedicated, and just as desirous of curing their patients as physicians are now. What they lacked then is the knowledge and technology that we have now that allow us to do what we do now. Medicine stagnated for hundreds of years, until the latter half of the 19th century, when it began to embrace science, and its failures tend to occur when it forgets science. Yet medicine advances nonetheless, thanks to science. It might do so in fits and starts. It might go down blind alleys. It might fall for fads based on less than rigorous science. But eventually, it advances, and we obtain the knowledge and develop the technology necessary to improve. Even in the fictional universe of Star Trek , I’d bet that the physicians of 1986 were no less clever and dedicated than Dr. McCoy. The difference is that Dr. McCoy had tricorders and other products of the science and technology of 2286. Science is what got us from the world of the Knick to where we are now, and science is what will get us to the world of Dr. McCoy.
Dr. Gorski's full information can be found here , along with information for patients. David H. Gorski, MD, PhD, FACS is a surgical oncologist at the Barbara Ann Karmanos Cancer Institute specializing in breast cancer surgery, where he also serves as the American College of Surgeons Committee on Cancer Liaison Physician as well as an Associate Professor of Surgery and member of the faculty of the Graduate Program in Cancer Biology at Wayne State University. If you are a potential patient and found this page through a Google search, please check out Dr. Gorski's biographical information, disclaimers regarding his writings, and notice to patients here .
View all posts
- Posted in: Cancer , History , Science and the Media , Surgical Procedures
- Tagged in: Angela Kester , Burns Archive , chemotherapy , James Kildare , John Thackery , Leonard McCoy , lobotomy , medical history , radical mastectomy , science based medicine , Spock , Star Trek , Star Trek IV: The Voyage Home , Steven Kester , Steven Soderbergh , surgery , The Knick , tricorder , William Halsted , William Stewart Halsted
Posted by David Gorski
- The Original Series
- The Animated Series
- The Next Generation
- Deep Space Nine
- Strange New Worlds
- Lower Decks
- Star Trek Movies
- TrekCore on Twitter
- TrekCore on Facebook
Let’s rewind a bit, though, so I can explain a bit about how one goes about making a 3D map of someone’s white matter. White matter is essentially the ‘cabling’ of your brain, carrying signals from the grey matter and relaying them to places like your muscles when you want to move. (Grey matter is what does your cognitive processing, gets upset, feels happy, receives signals, stores memories, makes decisions, and all that other wonderful stuff your brain gets up to.)
It also carries sensory information and allows the different bits of the brain to exchange information. If your brain was the internet, grey matter is the servers, white matter is the cabling which links them to the peripherals and end users.
Stamets’ brain scan shows the corpus callosum, which is a very large extruded U-shaped tract which allows the two hemispheres of the brain to talk to each other. The close-up is good enough to see that this is constructed with the streamline algorithm I just mentioned, and rendered using straight-line segments. It’s pretty well segmented — in fact, you can see lots of lateral connections, which are easily missed in tractography.
Tilly even states that the scan is showing “changes in gross white matter structure, caused by interactions with the mycelial network,” which is neat, because diffusion and tractography is exactly what you’d use to look for structural abnormality. I have to admit, though, that I haven’t seen a lot of work on diffusion MRI and the mycelial network — but conference season is starting up again, so you never know!
Here, you could compare Stamets’ scan to either a population average, or to earlier scans from his own brain taken before he took on tardigrade duty. It’s all right there — hats off to the show researchers.
Diffusion imaging a particular type of MRI which measures (you guessed it!) diffusion. The human body is full of fluids, and our brains sit in a bath of warm, salty water inside our skulls — and the water is always moving. The molecules jostle and bump into each other randomly and slowly move around in a more-or-less undirected way.
You might remember Brownian motion from high school; that’s the same phenomenon. Dust motes are jostled by the water and slowly spread out, and diffusion imaging allows us to measure how much jostling motion is going on — constructing an image which tells you how much jostling is happening in each pixel. The more jostling, the lower the signal and the darker the pixel.
We can do a lot better than simply ‘dark vs. light,’ though: one of the cool things about the technique is that you can do this in 3D, and get a picture of how things are moving in different directions, in each pixel. From there you can estimate which directions have the most diffusion, and which have the least. There’s a difference between the high school Brownian motion and diffusion in a brain, however: the brain gets in the way.
Diffusing particles don’t just bump into each other, they bump into other things in the tissue, like cell membranes, processing architecture, and cabling — something particularly interesting, because it points in a particular direction.
Imagine being inside a narrow pipe: you can move along the pipe in either direction, but it’s hard to move across it. Flip that around, and if you could measure the direction particles diffuse the furthest, you tell what direction the pipe was pointing. With 50 or 60 different measurements, you can do exactly that.
What’s more, you can do it separately in each and every pixel in the image, ending up with images that look a bit like these (courtesy of my friend Donald Tournier’s MRtrix software ):
If you look closely, you can see that there’s a little coloured blob in each pixel, which represents the diffusion in 3D. The peaks of the blobs are the directions of most diffusion. We can extract the directions corresponding to the peaks, and we’ve got our estimates of which direction the tissue points.
At this point, we’ve got a load of local orientations; a grid of tiny arrows which tell you which was diffusion is greatest. This works very nicely in cable-like structures like white matter, as we’re estimating local orientations and can even split out the directed tissue from the undirected fairly easily.
We’re not quite at Stamets’ scan yet, though, because there’s still one more thing to do: join those arrows together — this is called tractography . It starts with a 3D field of orientations, and builds up a set of continuous fibres.
There are actually a few different ways to do this, and some are more sophisticated than others, but one standard way is pretty much join-the-dots.
You pick a place to start, and then you follow the field by stepping along the local direction by a small distance, checking the new local orientation, turning in that direction and stepping on. You keep going until there no more directionality — or the structure takes a sharp turn, usually greater than 90 degrees.
Do this a few thousand times from a bunch of start points, and you can construct what’s called a tract — a big piece of white matter which looks like the sort of thing you’d find in a medical textbook — and with that in mind, we reach our lab’s version of Stamets’ brain scan:
This is a reconstruction of the corpus callosum using diffusion MRI and streamline tractography. It’s the same data from before, but with the streamlines built up. We’ve also added a 3D cortical surface from the same scan… which is there mostly to make it look cool. This isn’t Stamets’ brain, of course; it’s actually a scan of Kiran Seunarine, our resident tractography expert. (To the best of my knowledge, he’s not able to navigate the mycelial network yet…)
So if we’re not scanning for spore drive brain issues, why might you want to do this in real life? Well, one of the nice things about tractography is that it shows you the 3D structure in each individual patient, not just a textbook version of a brain. This might be interesting if you’re studying how brains change during aging or natural development, for example, but it’s also useful if something goes wrong: brain tumours, for example.
A growing tumour pushes the tissue around it aside or can grow right over the top of something else. If a surgeon is operating to remove it, the biggest risks are either not removing all or it — in which case it could grow back — or removing too much, taking some healthy tissue out as well.
There’s also the question of how you get to the thing in the first place. You want to avoid cutting through white matter, because once it’s gone, it’s gone — and a broken cable in the brain is like a broken cable in any other network. Information can’t get through, except in this case that blocked sensory information might be coming from your eyes or fingertips. You want that information to get through.
One of the things we do in our lab is tractography for neurosurgeons, used in reconstructing white matter around, say, a tumour, so the surgeons can use it to plan the procedure. The more information they can get, the better they can plan, and the better patients will recover.
Tilly also uses imaging to monitor how well a treatment is working, and we do that too. We also use diffusion imaging and tractography to look at brain maturation — from early childhood to adolescence — to learn more about what’s happening in healthy kids, and when they’re suffering from a disease like epilepsy or multiple sclerosis. There’s a lot you can tell from white matter.
Diffusion MRI technology is a little bit of 23rd century sickbay magic that’s actually already here. As far as I know, no one is using it to scan tardigrade brains quite yet, but I’m trying to see if my colleagues in the lab will let me render everything in Discovery’s pink and blue color scheme to bring that Starfleet feeling back down to Earth.
Matt Hall is a research scientist at University College London and the UK’s National Physical Laboratory working with advanced MRI technology to develop the tools needed to obtain the most detailed and accurate images possible of human tissue. He is part of a team of scientists and clinicians at The UCL Institute of Child Health who develop and apply new MRI methods, particularly for childhood illnesses.
The images in this article were created by Kiran Seunarine , a scientist with a background in design and visualisation — a modern-day Geordi La Forge who works with magnets instead of warp reactors.
- Diffusion MRI
- DSC Season 1
- Mycelial Network
- Star Trek: Discovery
- The Wolf Inside
Related Stories
New star trek: discovery — black alert strategy board game announced, win star trek: discovery’s first three seasons on blu-ray, star trek: discovery 3-season blu-ray collection announced, search news archives, new & upcoming releases, featured stories, star trek: lower decks cancelled; strange new worlds renewed for season 4, our star trek: discovery season 5 spoiler-free review, star trek: discovery’s final adventure begins in april 2024.
TrekCore.com is not endorsed, sponsored or affiliated with Paramount, CBS Studios, or the Star Trek franchise. All Star Trek images, trademarks and logos are owned by CBS Studios Inc. and/or Paramount. All original TrekCore.com content and the WeeklyTrek podcast (c) 2024 Trapezoid Media, LLC. · Terms & Conditions
June 16, 2017
How Close Are We to a Real Star Trek –Style Medical Tricorder?
Vital signs information and images aren’t enough for a fully automated device that can tell you what’s actually wrong with a patient
By Despina Moschou & The Conversation US
The following essay is reprinted with permission from The Conversation , an online publication covering the latest research.
Does science inspire fiction or does it work the other way around? In the case of medical technology, the long-running TV and film series Star Trek has increasingly been inspiring researchers worldwide. Two teams were recently awarded the Qualcomm Tricorder X Prize for developing handheld devices that can diagnose a range of diseases and check a patient’s vital signs without invasive tests – inspired by Star Trek’s medical “tricorder” device.
On supporting science journalism
If you're enjoying this article, consider supporting our award-winning journalism by subscribing . By purchasing a subscription you are helping to ensure the future of impactful stories about the discoveries and ideas shaping our world today.
In the show, a doctor would use the tricorder and its detachable scanner to quickly gather data on a patient and instantly work out what was wrong with them. It could check organ functions and detect diseases and their causes, and also contained data on a range of alien lifeforms. But how close are we really to using such devices (assuming we don’t need them to diagnose aliens)?
The main aim of the two prizewinners is to integrate several technologies in one device. They haven’t created an all-in-one handheld machine but they do both represent significant steps forward.
The main winner, known as DxtER and created by US firm Basil Leaf Technologies, is actually an iPad app with artificial intelligence. It uses a number of non-invasive sensors that can be attached to the body to collect data about vital signs, body chemistry and biological functions. The runner-up technology from Taiwan’s Dynamical Biomarkers Group similarly connects a smartphone to several wireless handheld test modules that can analyse vital signs, blood and urine, and skin appearance.
The judges said both devices nearly met the benchmarks for accurately diagnosing 13 diseases including anaemia, lung disease, diabetes, pneumonia and urinary tract infection. These are the most successful efforts we’ve seen to bring so many functionalities into a single, user-friendly, portable diagnostic system.
Part of the success is due to the development of a variety of technologies that make up such all-in-one systems, although they still have some way to go. Probably the most advanced are mobile vital signs monitoring devices. For example, the ViSi Mobile System can remotely monitor all core vital signs including blood pressure, blood oxygen, heart rate and electrical activity, and skin temperature. It uses electrocardiogram (ECG) sensors attached to the chest and a pressure sensor in cuffs on the thumb and arm, both attached to a wearable wrist unit that feeds all the signals wirelessly to desktop or mobile device, with the same accuracy as conventional intensive care equipment .
All the various sensor data from a system such as this then needs to be turned into meaningful readings – and that requires specialist software. For example, the Airstrip Technologies software can pull in information from hundreds of different types and brands of patient monitors and other equipment, as well as medical records, scan results and even messaging apps, to display a full picture of patient’s changing condition in real time.
Portable imaging technologies are another element needed to assess a patient and present the relevant information. For example, there are already miniaturized USB-based ultrasound probes that can connect directly to a smartphone to provide instant ultrasound images. With the quality of mobile cameras and image processing capabilities continually improving, this technology is likely to get even better in the near future. This could mean instant X-ray scans or skin abnormality diagnosis using pattern recognition software.
Data and diagnosis
But vital signs information and images aren’t enough for a fully automated device that can tell you what’s actually wrong with a patient. The most mature technology we have in this area is for diabetes monitoring. Portable home blood glucose meters that can test a drop of blood on a paper can already be connected to mobile apps to allow diabetes sufferers to assess the severity of their condition.
Meanwhile, completely non-invasive methods for measuring glucose that don’t involve finger pricking to get a drop of blood are under development. These include analysing sweat or the interstitial fluid located a few micrometres below the skin’s surface (above the pain-causing nerves).
A number of innovative companies around the world are focusing on using similar handheld systems to diagnose other diseases, including HIV, tuberculosis, bacterial infections and cardiovascular disease. These rely on the key enabling technology of microfluidics, which uses specially designed microchips to manipulate tiny amounts of liquid.
Commonly known as lab-on-a-chip technology , this allows you to reduce a complete clinical laboratory testing system to a device a few centimetres across. You can take a sample, prepare it for testing (for example by isolating bacteria in the blood) and identify and measure the microbe present.
But while there has been significant progress in the developing bits and pieces of a tricorder, there is still work to do putting them altogether in a genuinely handheld package. Various equipment needs to be miniaturised and we need more progress in portable computers so they can handle all the information and data required for a complete picture of a patient’s health condition. We also need more development of the more thorough diagnostic features, such as the lab-on-chip and portable imaging systems, and less invasive testing methods. We may not have a tricorder in our hands yet, but we are definitely getting closer.
This article was originally published on The Conversation . Read the original article .

How close are we to a real Star Trek-style medical tricorder?

Prize Fellow in Bioelectronics, University of Bath
Disclosure statement
Despina Moschou receives funding from the British Council-Newton Fund Institutional Links. She is also Managing Director and co-founder of the medical diagnostics company DxOnBoard Ltd.
University of Bath provides funding as a member of The Conversation UK.
View all partners
Does science inspire fiction or does it work the other way around? In the case of medical technology, the long-running TV and film series Star Trek has increasingly been inspiring researchers worldwide. Two teams were recently awarded the Qualcomm Tricorder X Prize for developing handheld devices that can diagnose a range of diseases and check a patient’s vital signs without invasive tests – inspired by Star Trek’s medical “tricorder” device.
In the show, a doctor would use the tricorder and its detachable scanner to quickly gather data on a patient and instantly work out what was wrong with them. It could check organ functions and detect diseases and their causes, and also contained data on a range of alien lifeforms. But how close are we really to using such devices (assuming we don’t need them to diagnose aliens)?
The main aim of the two prizewinners is to integrate several technologies in one device. They haven’t created an all-in-one handheld machine but they do both represent significant steps forward.
The main winner, known as DxtER and created by US firm Basil Leaf Technologies, is actually an iPad app with artificial intelligence. It uses a number of non-invasive sensors that can be attached to the body to collect data about vital signs, body chemistry and biological functions. The runner-up technology from Taiwan’s Dynamical Biomarkers Group similarly connects a smartphone to several wireless handheld test modules that can analyse vital signs, blood and urine, and skin appearance.
The judges said both devices nearly met the benchmarks for accurately diagnosing 13 diseases including anaemia, lung disease, diabetes, pneumonia and urinary tract infection. These are the most successful efforts we’ve seen to bring so many functionalities into a single, user-friendly, portable diagnostic system.
Part of the success is due to the development of a variety of technologies that make up such all-in-one systems, although they still have some way to go. Probably the most advanced are mobile vital signs monitoring devices. For example, the ViSi Mobile System can remotely monitor all core vital signs including blood pressure, blood oxygen, heart rate and electrical activity, and skin temperature. It uses electrocardiogram (ECG) sensors attached to the chest and a pressure sensor in cuffs on the thumb and arm, both attached to a wearable wrist unit that feeds all the signals wirelessly to desktop or mobile device, with the same accuracy as conventional intensive care equipment .
All the various sensor data from a system such as this then needs to be turned into meaningful readings – and that requires specialist software. For example, the Airstrip Technologies software can pull in information from hundreds of different types and brands of patient monitors and other equipment, as well as medical records, scan results and even messaging apps, to display a full picture of patient’s changing condition in real time.
Portable imaging technologies are another element needed to assess a patient and present the relevant information. For example, there are already miniaturized USB-based ultrasound probes that can connect directly to a smartphone to provide instant ultrasound images. With the quality of mobile cameras and image processing capabilities continually improving, this technology is likely to get even better in the near future. This could mean instant X-ray scans or skin abnormality diagnosis using pattern recognition software.
Data and diagnosis
But vital signs information and images aren’t enough for a fully automated device that can tell you what’s actually wrong with a patient. The most mature technology we have in this area is for diabetes monitoring. Portable home blood glucose meters that can test a drop of blood on a paper can already be connected to mobile apps to allow diabetes sufferers to assess the severity of their condition.
Meanwhile, completely non-invasive methods for measuring glucose that don’t involve finger pricking to get a drop of blood are under development. These include analysing sweat or the interstitial fluid located a few micrometres below the skin’s surface (above the pain-causing nerves).

A number of innovative companies around the world are focusing on using similar handheld systems to diagnose other diseases, including HIV, tuberculosis, bacterial infections and cardiovascular disease. These rely on the key enabling technology of microfluidics, which uses specially designed microchips to manipulate tiny amounts of liquid.
Commonly known as lab-on-a-chip technology , this allows you to reduce a complete clinical laboratory testing system to a device a few centimetres across. You can take a sample, prepare it for testing (for example by isolating bacteria in the blood) and identify and measure the microbe present.
But while there has been significant progress in the developing bits and pieces of a tricorder, there is still work to do putting them altogether in a genuinely handheld package. Various equipment needs to be miniaturised and we need more progress in portable computers so they can handle all the information and data required for a complete picture of a patient’s health condition. We also need more development of the more thorough diagnostic features, such as the lab-on-chip and portable imaging systems, and less invasive testing methods. We may not have a tricorder in our hands yet, but we are definitely getting closer.
- Medical devices
- Medical technology
- Vital signs
Faculty of Law - Academic Appointment Opportunities
Operations Manager
Senior Education Technologist
Audience Development Coordinator (fixed-term maternity cover)
Lecturer (Hindi-Urdu)
Chief medical officer
- View history

The Chief medical officer ( CMO ) was a senior staff position and was responsible for the maintenance of a crew's health and fitness. In a Starfleet unit, the officer also served as chief surgeon . The chief medical officer maintained and operated medical facilities of starships, stations, and planetary posts. The medical staff, including all medical officers and counselors, were overseen by the chief medical officer.
- 1 Duties and functions
- 3 Known Chief medical officers
- 4 External links
Duties and functions [ ]
The CMO was responsible for conducting routine physical examinations and special duty physicals. Other duties included diagnosing and treating any crew ailments, run emergency medical drills, train the crew in first aid, set up remote hospitals and clinics and, when possible, find cures for any new conditions encountered by the starship. Starfleet vessels were often tasked to render medical assistance to any ship, station, or planet in need, and the chief medical officer was charged with ensuring there application of said aid. A ship's CMO performed any needed medical procedures and any elective surgery as authorized. The officer coordinateed with the Head Counselor or executive officer with respect to the crew psychological well being. The chief medical officer prescribed special diets and exercise regimens as necessary. In regards to any special environments required by alien crewmembers or visitors, the officer coordinated with the chief operations officer . Another task assigned to the ship's doctor was to monitor the ship's food replicators to ensure proper nutrition and safety.
Due to the sensitivity and responsibility of the position, the chief medical officer was usually a Commander or a Lieutenant commander in rank. For smaller starships, the officers were of the rank of Lieutenant or Lieutenant junior grade .
Known Chief medical officers [ ]
- Lieutenant Commander Leonard McCoy - USS Enterprise , USS Enterprise -A
- Commander Beverly Crusher - USS Enterprise -D , USS Enterprise -E , USS Invincible
- Lieutenant Julian Bashir - Deep Space 9
- EMH aka "The Doctor" - USS Voyager
- Selar - USS Excalibur , USS Excalibur -A
- Edinger Deet - USS Sunnyvale ( 2370 )
- Uldo Osprin - USS Sunnyvale ( 2381 ), USS L'Étoile du Nord
- Span - USS Federalist
- Warragul Wirrpanda - USS Bajor
- Robert Dalton - USS Pioneer
- Michael Donaldson - USS Victory- D
- Kaycee Horton - USS Victory -D, USS Victory -E
- Zander Farrell - Deep Space 12
- Lieutenant Commander Lillian Crusher - USS Valiant
- Commander Savel - USS Enterprise -F
- Commander Dilalai Quinn - USS Marvel
- Lieutenant Commander Matthew Jones - USS Endurance
External links [ ]
- Chief medical officer article at Memory Alpha , the canon Star Trek wiki.
- Chief medical officer article at Memory Beta , the non-canon Star Trek wiki.
- Chief medical officer article at Star Trek Expanded Universe .
- 1 Invincible class
- 2 Valkyrie class (Vanguard)
- 3 USS Invincible (NCC-88777)
Screen Rant
Christopher collins' 4 star trek roles explained.
Comedian and actor Christopher Collins played four different characters in Star Trek: The Next Generation & Star Trek: Deep Space Nine.
- Christopher Collins portrayed multiple characters in Star Trek, including Captain Kargan and Captain Grebnedlog in TNG.
- Collins' portrayal of Markalian Durg in DS9 showed his diverse acting range in the Star Trek universe.
- Despite his brief appearances, Collins made a lasting impact on the franchise with his various roles.
Actor and stand-up comedian Christopher Collins played four different Star Trek characters in episodes of Star Trek: The Next Generation and Star Trek: Deep Space Nine . In TNG's "Matter of Honor," Collins appeared as the Klingon Captain Kargan, who butted heads with his temporary First Officer, Commander William Riker (Jonathan Frakes). Collins played another Captain in TNG's "Samaritan Snare," this time a Pakled named Grebnedlog. In DS9 , Collins appeared as Markalians in both of his appearances, one of whom was a mercenary named Durg, while the other was an unnamed guard.
Christopher Collins was an actor and comedian most known for his voice-over roles in animated projects. He provided the voice for Cobra Commander in several different versions of the animated G.I. Joe series. He also voiced Starscream and numerous other characters in the first Transformers animated series. In addition to his Star Trek appearances, Collins appeared in episodes of Doogie Howser, M.D., Seinfeld, NYPD Blue, and Married... with Children . He had a few minor film roles, including appearances in Road House, True Identity, and A Stranger Among Us . Collins also had a successful career in stand-up comedy and won the San Francisco International Stand-Up Comedy Competition in 1990. Tragically, Collins passed away in 1994 at the age of 44.
Christopher Collins originated the voice of Mr. Burns on The Simpsons , but had to turn over the role to Harry Shearer after only a few episodes. Shearer modeled his performance on that of Collins.
Every Upcoming Star Trek Movie & TV Show
4 captain kargan, star trek: the next generation season 2, episode 8 - "a matter of honor".
In Star Trek: The Next Generation 's "Matter of Honor," Commander Will Riker (Jonathan Frakes) participates in an officer exchange program and takes on the role of First Officer on the Klingon vessel, the Pagh. Christopher Collins portrays the Klingon commander of the Pagh, Captain Kargan, who is suspicious of Riker from the jump. When a strange bacteria is discovered on the Pagh's outer hull, Kargan suspects Captain Jean-Luc Picard (Patrick Stewart) and the USS Enterprise-D are responsible.
"A Matter of Honor" updated the Klingons for TNG and established their culture moving forward.
When Kargan refuses to listen to his temporary First Officer, Riker has Kargan beamed over to the Enterprise and takes over command of the Pagh. After the Enterprise helps repair the Pagh, Kargan returns to his ship and dismisses Riker for being insubordinate. Still, it's clear Kargan has developed a certain amount of respect for Riker, despite all of his Klingon bluster. With its depictions of life aboard a Klingon ship, "A Matter of Honor" updated the Klingons for TNG and established their culture moving forward.
3 Captain Grebnedlog
Star trek: the next generation season 2, episode 17 - "samaritan snare".
Christopher Collins' next Star Trek appearance came later in Star Trek: The Next Generation season 2 when he played Captain Grebnedlog, the commander of the Pakled ship Mondor. As Captain Picard heads to a nearby starbase for a medical procedure, Commander Riker is left in command of the USS Enterprise-D. The Enterprise soon receives a distress call from the Mondor, and Captain Grebnedlog tells Riker and his crew that the unintelligent Pakleds need help to make their ship go.
Commander Riker sends Lt. Geordi La Forge (LeVar Burton) over to help with repairs, but the Pakleds soon take Geordi as a hostage. While Grebnedlog and his crew may not be very intelligent, they have managed to gain technology by stealing it from other species. Riker makes some questionable decisions in "Samaritan Snare," but he does trick the Pakleds into releasing La Forge in the end.
The Pakleds did not appear on screen again until the animated Star Trek: Lower Decks , where their ridiculous but sometimes dangerous antics are a much better fit.
Star Trek: Deep Space Nine Season 1, Episode 9 - "The Passenger"
In Star Trek: Deep Space Nine’s “The Passenger,” Christopher Collins played Durg, a Markalian mercenary who met with the profit-hungry Ferengi Quark (Armin Shimerman). When a criminal Kobliad named Rao Vantika (James Harper) transfers his consciousness to Dr. Julian Bashir (Alexander Siddig), he employs Durg to help him steal a shipment of deuridium. Durg and his fellow mercenaries attack the freighter transporting the deuridium, the Norkova, killing the bridge crew and taking control of the ship.
The crew of space station Deep Space Nine then trap the Norkova with a tractor beam, but Vantika continues to try to escape. Still inhabiting the body of Dr. Bashir , Vantika orders Durg to jump to warp speed (which would destroy the freighter), but he refuses. Vantika then kills Durg, before Commander Benjamin Sisko (Avery Brooks) and Lt. Jadzia Dax (Terry Farrell) figure out a way to communicate with Bashir and resolve the situation.
1 Unnamed Markalian Guard
Star trek: deep space nine season 2, episode 19 - "blood oath".
Christopher Collins played another member of the Markalian species in DS9’s “Blood Oath. This Markalian served as an assistant and guard for the infamous criminal known as The Albino (Bill Bolender). Many years before, three Klingon warships were dispatched to capture the Albino, and while they managed to destroy his base, the Albino himself escaped. These three Klingon ships were led by Kor (John Colicos) , Koloth (William Campbell), and Kang (Michael Ansara). The Albino later retaliated by killing each of the Klingon’s firstborn sons, which prompted them to swear a blood oath to kill the Albino.
Kor, Koloth, and Kang all appeared as Klingons on Star Trek: The Original Series , and all three actors reprise their respective roles.
The three Klingons arrive on Deep Space Nine eighty-one years later, after Kang reveals he has discovered the Albino’s location. With the help of Jadzia Dax (whose former symbiote Curzon was godfather to Kang’s son), the three Klingons attack the Albino. After alerting the Albino to the presence of the Klingons, the guard is ultimately killed by Kang while the Albino cowers behind him. Although Kang manages to kill the Albino, he and Koloth both die from their wounds. With the three boisterous Klingons stealing the show, Collins’ Markalian guard does not make as much of an impression, but he nevertheless left his mark on the Star Trek franchise.
Star Trek: The Next Generation
Star trek: deep space nine.

Barbara Baldavin, ‘Star Trek,’ ‘Medical Center’ actress, dead at 85
A ctress Barbara Baldavin, who appeared in three episodes of the original “ Star Trek ” television series during its first season and later appeared on “ Medical Center ,” died Sunday. She was 85.
>> Read more trending news
Baldavin died of congestive heart failure at her home in Manhattan Beach, California, her son, Marc D’Agosta, told The Hollywood Reporter . She was born on Oct. 18, 1938, the entertainment news website reported.
In the original “Star Trek” series, Baldavin played phaser control officer Angela Martine in two episodes, according to IMDb.com . During the series’ final season, she returned as Lt. Lisa in “Star Trek’s” last episode, according to The Hollywood Reporter .
Baldavin also appeared in 48 episodes of “Medical Center” from 1970 to 1976 as Nurse Holmby, according to IMDb.com . She played the character of Norma Summers in three episodes during the show’s first season in 1969.
She also had guest roles on “Rawhide,” “The Fugitive,” “Insight,” “Columbo,” “Mannix,” “Adam-12,” “Toma,” “The F.B.I.,” “McMillan & Wife,” “Bronk,” “Baretta,” “Charlie’s Angels,” “Barnaby Jones,” Vega$” and “Fantasy Island,” according to The Hollywood Reporter .
During the 1980s, Baldavin worked in the casting departments of several television shows, including “Hagen,” “Square Pegs,” “Matt Houston,” “Dynasty,” “Finder of Lost Loves” and “Trapper John, M.D., according to The Hollywood Reporter .

The Definitive Voice of Entertainment News
Subscribe for full access to The Hollywood Reporter
site categories
Barbara baldavin, actress on ‘star trek’ and ‘medical center,’ dies at 85.
She later was involved in casting on such series as ‘Dynasty,’ ‘Matt Houston’ and ‘Trapper John, M.D.’
By Mike Barnes
Mike Barnes
Senior Editor
- Share this article on Facebook
- Share this article on Twitter
- Share this article on Flipboard
- Share this article on Email
- Show additional share options
- Share this article on Linkedin
- Share this article on Pinit
- Share this article on Reddit
- Share this article on Tumblr
- Share this article on Whatsapp
- Share this article on Print
- Share this article on Comment

Barbara Baldavin, who appeared on three episodes of the original Star Trek and recurred on Medical Center before working in the casting department on shows including Dynasty and Trapper John, M.D. , has died. She was 85.
Baldavin died Sunday of congestive heart failure at her home in Manhattan Beach, her son Marc D’Agosta told The Hollywood Reporter .
Related Stories
Rico wade, outkast producer and organized noize member who co-founded the dungeon family collective, dies at 52, william shatner on living boldly throughout acting career: "the future is unheralded".
She then returned as Lt. Lisa, a communications officer and court reporter, on the series finale, “Turnabout Intruder,” which aired in June 1969.
Baldavin played Nurse Holmby on 51 episodes during the last six seasons (1970-76) of CBS’ Medical Center , starring Chad Everett and James Daly. She had appeared as another character on the first season.
In the 1980s, she worked in the casting departments of shows including Hagen — Everett’s series follow-up to Medical Center — Square Pegs , Matt Houston , Dynasty , Finder of Lost Loves and Trapper John, M.D.
A native of Quincy, Massachusetts, Baldavin started acting while attending El Camino College in Torrance, California, and she studied at the Lee Strasberg Institute.
She also showed up on episodes of Rawhide , The Fugitive , Insight , Columbo , Mannix , Adam-12 , Toma , The F.B.I. , McMillan & Wife , Bronk , Baretta , Barnaby Jones , Charlie’s Angels , Fantasy Island , Vega$ and more.
Baldavin worked as an instructor at Dawn Wells ‘ Film Actor’s Boot Camp. She and the late Gilligan’s Island star were great friends and shared a birthdate: Oct. 18, 1938.
Survivors include another son, Joseph, and her grandchildren, Casandra and Justine. Her former husband was Joseph D’Agosta, who served as casting director on Star Trek and other Desilu series.
THR Newsletters
Sign up for THR news straight to your inbox every day
More from The Hollywood Reporter
Science takes center stage at the 2024 breakthrough prize ceremony, o.j. simpson death could change equation for goldman, brown civil suit payouts, a lawsuit, a porn mogul and a ‘pawn stars’ cameo: the bizarre afterlife of o.j. simpson’s white bronco, george and amal clooney on “war on truth,” arizona abortion ban, ron goldman’s family calls o.j. simpson’s death “a mixed bag of complicated emotions”, adam levine reacts to mick jagger dancing to maroon 5 hit “moves like jagger”: “really surreal”.
2024 Election Trump held a rally in Pennsylvania, his last scheduled event before Monday’s trial.
- Share full article

Michael Gold
Donald Trump at a rally in Pennsylvania just endorsed Dave McCormick, who is expected to be the Republican candidate for Senate in the state. In 2022, Trump criticized McCormick, who was running against the candidate then preferred by the former president, Mehmet Oz

Shane Goldmacher
President Biden has shrunk former President Donald Trump’s lead to one percentage point in the latest New York Times/Siena College poll . How did he do it? Largely it appears by coalescing Democrats. Biden is now winning 89 percent of his 2020 supporters compared with 83 percent in February.

Ruth Igielnik
In our new poll, a little under half of voters think Trump should be found guilty in the 2016 campaign sex scandal cover-up case in New York, but very few are paying attention. Just a quarter of them say they’re paying a lot of attention, and about half describe the case as very serious. When others have polled on the seriousness of Trump’s four major criminal trials, this case often polls as the least serious.
In a new New York Times/Siena College poll , nearly equal shares of voters — a little under 60 percent — say Trump and Biden are a risky choice for president.
Biden’s improvement in our poll since February is correlated with a downtick in the share of voters saying he is too old to be an effective president. Most of that change comes from voters over 65, who are 17 percentage points less likely to be concerned about Biden’s age than they were in February.
In our latest Times/Siena poll , voters gave former President Donald Trump higher marks on how he handled the economy, immigration and foreign conflicts while in office than they did President Biden. Voters generally thought Biden did a better job of handling the coronavirus pandemic and unifying the United States than Trump did.
Our new Times/Siena poll finds a tight race, where former President Donald Trump has a narrow edge over President Biden. But Biden has closed the gap with Trump since February and consolidated support among his 2020 voters.

Neil Vigdor
Another 28 Democratic delegates are at stake on Saturday for President Biden, in Wyoming and Alaska, two sparsely populated states that are Republican strongholds. The last time a Democrat carried either one was in the 1964 presidential election, when Lyndon B. Johnson won both in his landslide victory over Barry Goldwater.

Nicholas Nehamas
Seth MacFarlane, the creator of “Family Guy,” hosted a fund-raiser for the Biden campaign at his Beverly Hills home on Friday, bring in about $1.5 million. He cracked a joke at the expense of the guests of honor, Vice President Kamala Harris and her husband, Doug Emhoff. “Anyway, now I wanted to get everything right to this introduction,” MacFarlane said. “So I practiced how to pronounce your name. Is it ‘Doug’?”

Annie Karni
Speaker Mike Johnson got everything he was hoping to get out of his trek to Mar-a-Lago on Friday: as full-throated an endorsement from Donald Trump as he could expect under the circumstances, which include a motion to oust him from his position by one of Trump’s most stalwart allies in the House. “I stand with the speaker” is what Trump said and what Johnson wanted his members to hear.
Vice President Kamala Harris laid into former President Donald Trump at a campaign rally on abortion rights in Tucson, Ariz. on Friday, framing the debate as an essential fight over freedom and women’s medical care. “Donald Trump is the architect of this healthcare crisis,” Harris said.
Donald Trump, explaining his changed stance on a federal abortion ban, said on Friday: “We broke Roe v. Wade. We did something that nobody thought was possible — we gave it back to the states.” At the same time, he said he disagreed with the Arizona court ruling this week that restored an 1864 law banning abortion.

Chris Cameron
Trump rallied in Pennsylvania, his last before his New York criminal trial begins.
Former President Donald J. Trump was in Pennsylvania on Saturday for a rally in Schnecksville, his last scheduled campaign event before his criminal trial in New York begins on Monday.
For more than a year, Mr. Trump has been shadowed by felony cases related to actions he took before, during and after his presidency. Alvin L. Bragg, the district attorney in Manhattan, indicted Mr. Trump on 34 felony counts of falsifying business records in the first degree, accusing him of covering up a sex scandal surrounding the 2016 presidential campaign.
The former president faces dozens of additional felony charges in three other criminal cases, all of which remain in pretrial proceedings. At least one of those cases could go to trial before the general election in November.
Mr. Trump spent the week before the start of his New York trial in retreat on his abortion policy. On Monday, he made a firm commitment that abortion policies should be left to the states and that “whatever they decide must be the law of the land.”
By Friday, Mr. Trump was openly criticizing strict bans in states like Florida and Arizona, and he said on social media that the Arizona State Legislature should “ACT IMMEDIATELY” to change a near-total abortion ban in the state that was enacted in 1864. The state’s top court upheld the ban in a ruling on Tuesday.
Vice President Kamala Harris, who held a rally in Tucson, Ariz., on Friday, excoriated Mr. Trump for what she and the Biden campaign have said is his direct responsibility for the strict abortion bans being enacted in some states. Ms. Harris highlighted Mr. Trump’s repeated boasting that he is “proudly the person responsible” for overturning the constitutional right to abortion once enshrined in Roe v. Wade. Nearly simultaneously from his private residence in Palm Beach, Fla., Mr. Trump bragged about his role once again.
“We broke Roe v. Wade,” he said during a joint news conference with the speaker of the House, Mike Johnson, Republican of Louisiana. “We did something that nobody thought was possible.”
The fallout from the Arizona Supreme Court’s decision comes as a New York Times/Siena College poll taken this week found that Mr. Biden had nearly erased Mr. Trump’s early polling advantage in the presidential race amid signs that some in the president’s base have come around to supporting him. The two candidates are now virtually tied, with Mr. Trump holding a 46 percent to 45 percent edge.
Kristi Noem, the South Dakota governor and Trump V.P. contender, is barred from tribal lands.
Four of South Dakota’s federally recognized Native American tribes have barred the state’s governor, Kristi Noem — a Republican whose name has been floated as a potential running mate for former President Donald J. Trump — from their reservations. The latest blocked Ms. Noem on Thursday .
Three of the tribes barred Ms. Noem this month, joining another tribe that had sanctioned the governor after she told state lawmakers in February that Mexican drug cartels had a foothold on their reservations and were committing murders there.
Ms. Noem further angered the tribes with remarks she made at a town hall event last month in Winner, S.D., appearing to suggest that the tribes were complicit in the cartels’ presence on their reservations.
“We’ve got some tribal leaders that I believe are personally benefiting from the cartels being there, and that’s why they attack me every day,” Ms. Noem said.
The tribes are the Cheyenne River Sioux, the Rosebud Sioux and the Standing Rock Sioux and the Oglala Sioux, which in February became the first group to bar Ms. Noem from its reservation. Their reservations have a combined population of nearly 50,000 people and encompass more than eight million acres, according to state and federal government counts. Standing Rock Indian Reservation, the third tribal area to have restricted Ms. Noem’s access, extends into North Dakota.
The tribes have accused Ms. Noem of stoking fears and denigrating their heritage when she referred to a gang known as the Ghost Dancers while addressing state lawmakers and said that it had recruited tribal members to join its criminal activities.
The gang has the same name as the participants in the Native American ghost dance ceremony , a sacred ritual dating to the 19th century.
“Gov. Kristi Noem’s wild and irresponsible attempt to connect tribal leaders and parents with Mexican drug cartels is a sad reflection of her fear-based politics that do nothing to bring people together to solve problems,” Janet Alkire, the chairwoman of the Standing Rock Sioux Tribe, said in a statement this week.
Ms. Noem stood by her comments in a statement to The New York Times on Friday.
“Tribal leaders should immediately banish the Mexican drug cartels that are responsible for murders, rapes, drug addiction and many more crimes on tribal lands,” she said. “The people in the communities live with unspeakable horrors and tragedy every day, but banishing me for telling the truth about the suffering does nothing to solve the problems. It may play well for the leftist media, but in reality, it’s pointless.”
When asked about Ms. Noem’s claims that tribal leaders were benefiting from the cartels’ presence on reservations, an aide pointed to her recent remarks to The Dakota Scout , an alternative newspaper based in Sioux Falls, S.D., doubling down on them and criticizing the tribes’ response to the cartels.
“That tells me that they are tied to them or benefiting from them somehow, that they’re allowing them to stay in their communities,” she said.
The governor’s office provided photos to The Times that it said were from a gang promotion ceremony featuring several men wearing clothing adorned with Ghost Dancers patches. The Times was unable to verify the images independently.
It also released a recording of a conversation that it said was between the secretary of the South Dakota Department of Tribal Relations and a leader of the Standing Rock Sioux Tribe in which they discussed how a single Tribal Council representative from South Dakota had voted to bar Ms. Noem from its reservation. The remaining votes came from Tribal Council members who reside in North Dakota, according to the governor’s office.
Efforts to reach the Tribal Council member said to be in the recording were not immediately successful.
In a social media post on Thursday, Ms. Noem argued that her comments about cartel activity on the reservations were similar to remarks that Senator Jon Tester, Democrat of Montana, made last month before the Senate Indian Affairs Committee.
“We’ve got cartels in Indian Country,” he said, using an expletive to say there was a lot of “bad” stuff going on.
Mr. Tester, a member of the Indian Affairs Committee, had been pushing for additional law enforcement resources for tribal lands, mirroring calls from tribal leaders in Montana for help from the federal government in addressing crime. His comments differed in tenor from Ms. Noem’s, and he did not level accusations that tribal leaders were complicit in the rise of the cartels on reservations.
A spokesman for Mr. Tester, who is running for re-election in a crucial contest for control of the Senate, declined to comment on Friday.
In November, the Oglala Sioux Tribe, citing a rise in drug-related offenses, assaults and homicides on its reservation, declared a state of emergency , which remains in effect.
Then, in January, the tribe accused the federal government in a lawsuit of failing to provide adequate funding as required by longstanding treaties for law enforcement coverage on the reservation, an area larger than Rhode Island and Delaware combined.
The tribe said in its lawsuit that it receives enough federal funding for only 33 police officers and eight criminal investigators, which it said had contributed to an uptick in crime. But the tribe pushed back against Ms. Noem’s claims that the cartels were using the reservation to facilitate the spread of illegal drugs and said that the problem existed when Mr. Trump was president.
The cartels’ reach on tribal lands is gaining heightened attention on Capitol Hill, where at least two congressional panels recently focused on surging crime connected to the groups.
At a hearing on Wednesday, Jeffrey Stiffarm, a tribal leader from Montana, told a House oversight committee that “these drug cartels are specifically targeting Indian Country because of a dangerous combination of rural terrain, history of addiction, under-resourced law enforcement, legal loopholes, sparsely populated communities and exorbitant profits, and it is devastating tribal reservations.”
South Dakota has nine federally recognized Native American tribes, which have at times sparred with Ms. Noem over issues related to their sovereignty , her support for the now-halted Keystone XL pipeline and access to their reservations at the start of the coronavirus pandemic.
The president of the Oglala Sioux Tribe, which in 2019 lifted a previous barring of her, said the governor’s political ambitions had motivated her actions.
In a statement posted on Facebook in February, the president, Frank Star Comes Out, said that “the truth of the matter is that Governor Noem wants the use of the so-called ‘invasion’ of the southern border as a Republican ‘crisis’ issue” to encourage Mr. Trump to use it as a campaign issue and to select her as his running mate.
At the Conservative Political Action Conference later in February, a straw poll showed Ms. Noem tied for the top choice to be Mr. Trump’s running mate .
The tribes’ criticism of Ms. Noem began after the governor addressed a joint session of the South Dakota Legislature on Feb. 2 about the tide of illegal border crossings.
“Make no mistake, the cartels have a presence on several of South Dakota’s tribal reservations,” she said. “Murders are being committed by cartel members on the Pine Ridge Reservation and in Rapid City, and a gang called the Ghost Dancers are affiliated with these cartels. They have been successful in recruiting tribal members to join their criminal activity.”
Ms. Noem said the state government did not have the jurisdiction to intervene and provide law enforcement support to South Dakota’s tribes.
On Thursday, Ms. Noem announced that South Dakota would begin offering training to tribal law enforcement officers , who currently must travel to New Mexico for it.
Reporting from Tucson, Ariz.
Harris blasts Trump on abortion at a campaign rally in Arizona.
Harris blasts trump on abortion in arizona, during a campaign rally, vice president kamala harris blamed former president donald j. trump for the arizona supreme court’s ruling to uphold a near-total ban on abortion..
What has happened here in Arizona is a new inflection point. It has demonstrated once and for all that overturning Roe was just the opening act. Just the opening act of a larger strategy to take women’s rights and freedoms. Part of a full-on attack — state by state — on reproductive freedom. And we all must understand who is to blame. Crowd: “That’s right.” Former President Donald Trump did this. Here’s what a second Trump term looks like. More bans, more suffering and less freedom. Just like he did in Arizona, he basically wants to take America back to the 1800s. Crowd: “That’s right.“ But we are not going to let that happen. [crowd cheering]

Vice President Kamala Harris laid into former President Donald J. Trump over abortion rights at a campaign rally in Arizona on Friday, accusing him of being directly responsible for a court decision this week that upheld the state’s 160-year-old near-total ban on abortion.
“Overturning Roe was just the opening act,” Ms. Harris told a crowd of several dozen supporters at a community center in Tucson, Ariz. “Just the opening act of a larger strategy to take women’s rights and freedoms. Part of a full-on attack — state by state — on reproductive freedom. And we all must understand who is to blame: Former President Donald Trump did this.”
Ms. Harris went on to call abortion restrictions in states like Arizona “Trump’s abortion bans.”
This week, the Arizona Supreme Court ruled that an 1864 law banning almost all abortions, without exceptions for rape or incest, could be enforced, although not right away. Doctors could face prosecution under the law, which dates to a time before Arizona became a state.
The court’s decision came the day after Mr. Trump said that abortion should be left to the states, underscoring the unfavorable political terrain for Republicans on the issue. As president, Mr. Trump appointed three of the Supreme Court justices who voted to overturn Roe v. Wade in 2022, which has led to a proliferation of abortion bans across red states.
Democrats, led by Ms. Harris, have seized on the Arizona law. The Biden campaign released a new messaging campaign with the tagline: “Donald Trump did this.” Abortion rights groups in Arizona have set up rallies around the state, which has a race for an open Senate seat this year that could determine control of the chamber.
“This has been a very, very scary week for our state of Arizona,” said Representative Ruben Gallego, a Democrat who is running for that Senate seat against Kari Lake, a Republican. “Tuesday’s decision rocked all of us. We now have the nation’s most extreme abortion ban.”
Democratic candidates nationwide are focusing on abortion in their races, buoyed by the knowledge that the issue has propelled their party to a series of unexpected victories over the last two years. Abortion is one of the few issues on which President Biden polls better than Mr. Trump.
Mr. Trump has said he does not support the Arizona law, as well as other extreme restrictions such as a six-week ban in Florida. He has argued that supporting those bans is hurting Republicans at the ballot box. But his allies have made plans to use the federal government to limit abortion should they win the White House. In Tucson, Ms Harris referred to those plans, which The New York Times has reported would rely on enforcing the Comstock Act .
“Here’s what a second Trump term looks like,” Ms. Harris said. “More bans, more suffering and less freedom. Just like he did in Arizona, he basically wants to take America back to the 1800s.”
“Shame!” the crowd cried out as she described the potential impact of the 1864 law.
For Ms. Harris, the prominence of abortion in the presidential race is a chance to expand her profile as vice president, as well as her presence on the campaign trail. Last month, she became the highest-ranking U.S. official known to visit an abortion clinic.
“Kamala Harris has become the abortion czar of the Biden administration,” Carol Tobias, the president of the National Right to Life Committee, an anti-abortion group, said in a statement. “Instead of joining with the pro-life movement to build programs and safety nets to help promote real solutions for women and their preborn children, Joe Biden and Kamala Harris have engaged in fear-mongering and propaganda.”
Ms. Harris may make for a more natural messenger on abortion than Mr. Biden, an 81-year-old practicing Catholic who has long expressed personal discomfort with the procedure even as he has become a committed supporter of abortion rights. He rarely uses the word “abortion” when speaking. On Friday, in contrast, Ms. Harris leaned into the issue.
In the United States, she argued, freedom includes the right “to make decisions about one’s own body and not have the government telling people what to do.”
Lisa Lerer contributed reporting.
On this, Trump and Biden agree: Trump killed Roe v. Wade.
President Biden and former President Donald J. Trump have widely divergent stances on abortion.
But they agree on one point: Mr. Trump was personally responsible for ending the constitutional right to abortion once enshrined in Roe v. Wade . And they are both eager to remind voters of that fact, over and over and over.
“We broke Roe v. Wade,” Mr. Trump said during a joint news conference with House Speaker Mike Johnson in Palm Beach, Fla., on Friday. “We did something that nobody thought was possible.” Minutes later, Mr. Biden’s campaign attacked Mr. Trump simply by amplifying that boast on social media .
The back and forth has become an increasingly frequent occurrence on the campaign trail in recent weeks. Even as Mr. Trump has made efforts to distance himself from the stricter limits on abortion that some states, including Arizona and Florida , have enacted after Roe was overturned in 2022, he has continued to remind voters of his role in an objectively unpopular aspect of his White House legacy.
Democrats are eager to promote Mr. Trump’s bragging over his role in ending the constitutional right to abortion. The Biden campaign in particular has often published posts on social media that are little more than a picture of the former president and a quotation from him saying that he “was able to kill Roe v. Wade.”
Polls have repeatedly found that most Americans disagree with the Supreme Court’s decision to overturn Roe , and Democratic candidates have won races across the country by focusing on abortion rights and Republicans’ efforts to curtail them .
Mr. Trump has acknowledged that Democrats have a clear electoral advantage when running on abortion, and he has repeatedly complained that Republicans do not know how to talk about the issue .
But Mr. Trump is encountering his own difficulties in speaking on the issue. On Monday, he said that abortion should be left to the states , and that “whatever they decide must be the law of the land.” On Wednesday, he went further, saying he would not sign a federal abortion ban if elected president. Early on Friday, he posted a message on social media urging Republicans in the Arizona State Legislature to “ACT IMMEDIATELY” to change a near-total abortion ban in the state that was enacted in 1864.
Hours later, he was back to bragging about his hand in overturning Roe.
“If you look at what we’ve done with Roe v. Wade,” Mr. Trump said at his news conference with Mr. Johnson, “we did something that everyone said couldn’t be done, and we got it done. I give great credit to the Supreme Court justices for having the courage to do it.”
Advertisement
General Orders and Regulations
- View history
Starfleet Command General Orders and Regulations were a series of guidelines used to instruct members of Starfleet on the proper etiquette and policy in a situation that required consultation for a resolution. These protocols were the foundation of Starfleet and the responsibility of its officers to uphold and protect, ranging from all manners of duty , such as interstellar diplomacy to punctuation of reports . Violations of protocol could have led to being placed on report , a court martial , demotion of rank , or other reprimands.
These guidelines' fundamental principles were integral for Starfleet officers to help avoid conflicts of interest, ( TNG : " Redemption ") including one's duty to the truth. ( TNG : " The First Duty ") Guidelines were useful in many situations, including when flag officers could not be consulted to resolve a situation. ( VOY : " Equinox ")
Several of the first one-hundred-plus Starfleet Orders were used by the United Earth Starfleet prior to the founding of the Federation . ( ENT : " Hatchery ")
No Starfleet regulations permitted one's execution without a trial , something Spock reminded James T. Kirk of in 2259 of the alternate reality . The first officer was expressing his concerns about Kirk hunting down and assassinating " John Harrison ". He also added that a preemptive strike on Qonos was not permissible either. Kirk reminded him that their orders from Admiral Alexander Marcus was not a matter of Starfleet regulation. Spock then reminded him that apart from regulations, the act would be immoral . Kirk then countered that by saying that regulations aside, rescuing Spock from the volcano on Nibiru was moral, yet nobody congratulated him for doing so. ( Star Trek Into Darkness )
As of 2366 , there were no regulations prohibiting the unauthorized recreation of Starfleet personnel on the holodeck . ( TNG : " Hollow Pursuits ")
In 2373 , Captain Kathryn Janeway joked with Commander Chakotay about Ensign Hickman imitating her. " Imitating the captain, huh? Surely that violates some kind of Starfleet protocol. " ( VOY : " Scorpion ")
- 1 Starfleet Charter Articles
- 2 Federation Regulations
- 3 Galactic Emergency Procedures
- 4 General Orders
- 5 Starfleet Directives
- 6 Starfleet labor code
- 7 Starfleet Orders
- 8 Starfleet Regulations
- 9 Starfleet Away Team Guidelines
- 10 Starfleet Equipment Protocols
- 11 Starfleet Intelligence Procedures
- 12.1 See also
- 13 Starfleet Safety Protocols
- 14 Starfleet Security Protocols
- 15 Starfleet Temporal Protocols
- 16 Starfleet Transfer Regulations
- 17 Starfleet Treaty Protocols
- 18 Starfleet/Federation Codes
- 19.1 Health-related
- 19.2 Relationships
- 19.3 Miscellaneous
- 20 Fictional
- 21.1.1 "The only death penalty"
- 21.2 Apocrypha
- 21.3 See also
- 21.4 External link
Starfleet Charter Articles [ ]
- Article 14, Section 31: The exact language has never been cited, but certain lines in this section permitted the use of "extraordinary measures" in times of dire emergency. ( ENT : " Divergence ")
Federation Regulations [ ]
- Book 19, Section 433, Paragraph 12: Regulation concerning the ability of ranking Federation officials to give direct orders to Starfleet officers. This regulation was referred to but not cited by High Commissioner Ferris in 2267 , during a search for the then-missing shuttlecraft Galileo . ( TOS : " The Galileo Seven ")
Galactic Emergency Procedures [ ]
- Title 15 of these procedures allowed ranking Federation officials to assume direct command of Starfleet vessels under certain conditions. ( TOS : " The Galileo Seven ")
General Orders [ ]

General Order 1, Section 1

General Order 1, Section 2
- General Order 1: " No starship may interfere with the normal development of any alien life or society. " ( TAS : " The Magicks of Megas-Tu ") In 2259 , the Federation Council renamed General Order 1 the Prime Directive , a title by which it later became better known. ( SNW : " Strange New Worlds "; TNG : " The Drumhead "; PRO : " First Con-tact ") It superseded all other laws and directives, with the exception of the Omega Directive . ( VOY : " The Omega Directive ") Sections 1 and 2 specifically read:
Section 1: Starfleet crew will obey the following with any civilization that has not achieved a commensurate level of technological and/or societal development as described in Appendix 1. No identification of self or mission. No interference with the social, cultural, or technological development of said planet. No references to space, other worlds, or advanced civilizations. The exception to this is if said society has already been exposed to concept, herein. However, in that instance, section 2 applies. Section 2: If said species has achieved the commensurate level of technological and/or societal development as described in Appendix 1, or has been exposed to the concepts listed in section 1, no Starfleet crew person will engage with said society or species without first gathering extensive information on the specific traditions, laws, and culture of that species civilization. Then Starfleet crew will obey the following: If engaged with diplomatic relations with said culture, will stay within the confines of culture's restrictions. No interference with the social development of said planet.
- General Order 4: Though stated in 2269 (stardate 5928.5) that " Starfleet expressly forbids the death penalty ", this general order was stated to be the " only one exception ", and as such, mutiny was not considered to be in violation of this order. ( TOS : " Turnabout Intruder ")
- General Order 5: An order that prohibits Starfleet officers from, for example, transporting out of a dangerous situation if others would be put at risk by doing so. ( LD : " Second Contact ")
- General Order 6: If all life aboard a Federation starship had perished at the end of twenty-four hours, the ship would self-destruct to protect other beings from the disease on board. ( TAS : " Albatross ")
- General Order 7 : No vessel under any condition, emergency or otherwise, is to visit Talos IV . This was also said to have been " the only death penalty left on our books ". ( TOS : " The Menagerie, Part I ") When broken by Spock in 2267 , Commodore José I. Mendez , speaking for Starfleet, issued the following statement: " In view of historic importance of Captain Pike in space exploration, General Order 7 prohibiting contact Talos IV is suspended this occasion. No action contemplated against Spock. Proceed as you think best. " ( TOS : " The Menagerie, Part II ") In 2328, Talos IV was the destination for passengers traveling from Triskelion Orbital Station via commercial transport. Ryan Adams, Wynsdey Adams, Loren Bivens, and Svetlana Reeves-Stevens traveled on the SS Kogin , and Mike Echols traveled on the SS Wisconsin . ( TNG-R : " Inheritance ", okudagram )

General order 12 in effect (right)
- General Order 12: " On the approach of any vessel, when communications have not been established… " This order began to be cited by Saavik in 2285 , but she was interrupted before she could complete her quotation of the order. ( Star Trek II: The Wrath of Khan ) In 2401 , General Order 12 was referenced on screen for Anton Chekov 's presidential message. ( PIC : " The Last Generation ")
- General Order 13: Evacuation order for Starfleet vessels. ( Star Trek )
- General Order 15: "No flag officer shall beam into a hazardous area without armed escort." When Saavik cited this order in 2285, Kirk replied, "There's no such regulation!" ( Star Trek II: The Wrath of Khan )
- General Order 24: An order to destroy all life on an entire planet . This order has been given by Captain Garth on Antos IV and Captain Kirk on Eminiar VII . On neither occasion was the order actually fulfilled. ( TOS : " Whom Gods Destroy ", " A Taste of Armageddon ")
Starfleet Directives [ ]
- Directive 010: " Before engaging alien species in battle, any and all attempts to make first contact and achieve nonmilitary resolution must be made. " ( VOY : " In the Flesh ", ST : " Ask Not ")
- Directive 101: Any individual accused of a crime does not have to answer any questions. ( VOY : " Meld ")
- Tactical Directive 36: " The captain will not engage a hostile force without the protection of a security officer . " ( VOY : " Unimatrix Zero ")
- Prime Directive : Personnel should refrain from interfering with the developement of non-warp capable species. Reference to General Order 1 for details.
- Omega Directive : Authorizes the use of any and all means to destroy an Omega molecule. ( VOY : " The Omega Directive ")
- Temporal Prime Directive : Personnel are strictly forbidden from directly interfering with historical events.
Starfleet labor code [ ]
- Section 48, Alpha-7 : Requires meal breaks at regular intervals. This was a regulation for at least 122 years, from 2259 to 2381 . ( SNW : " Those Old Scientists ")
Starfleet Orders [ ]
- Starfleet Order 2: Starfleet regulation against the taking of intelligent life. ( TAS : " One of Our Planets Is Missing ")
- Section B, Paragraph 1-A – In the absence of a starship's assigned captain, a flag officer had the authority to assume command of the starship should they have deemed it necessary. ( TOS : " The Doomsday Machine "; VOY : " Tinker Tenor Doctor Spy ")
- Section C – Should it be proven with admissible evidence that the flag officer who had assumed command was medically or psychologically unfit for command, the starship's ranking officer could relieve them on that basis. However, such an action was required to be supported by an appropriate certification of unfitness by the ship's chief medical officer (requiring the CMO to also produce test results to that effect) or other clear evidence, such as an act of attempted suicide ( TOS : " The Doomsday Machine "), or other odd behavior. ( ENT : " Hatchery "; ; VOY : " Tinker Tenor Doctor Spy "; PRO : " Supernova, Part 1 ")
- Starfleet Order 2005: Orders the destruction of a starship by allowing matter and antimatter to mix in an uncontrolled manner. This was a last resort for a captain that allowed them to prevent their ship or crew from falling into enemy hands. ( Star Trek: The Motion Picture ) Admiral James T. Kirk executed this order (without directly citing it) when he ordered his officers to initiate the Enterprise 's self-destruct sequence.
- Starfleet Order 28455: Federation order that dictated the formal relief of a commanding officer by their successor. In the alternate reality , Admiral Richard Barnett told Captain James T. Kirk that, per this order, he had to report to Admiral Christopher Pike to relieve him of command of the Enterprise . ( Star Trek )
- Special Order 66715: Federation order that stated, " [Starfleet has] the authority to neutralize security threats to Deep Space 9 by any means necessary. " ( DS9 : " Inquisition ")
Starfleet Regulations [ ]
- Regulation 3 , Paragraph 12: In the event of imminent destruction, a Starfleet captain was authorized to preserve the lives of his crew by any justifiable means. Captain Ransom attempted to use this regulation to convince Captain Janeway that actions he took against a species of nucleogenic lifeforms were justified, but Janeway doubted that the regulation covered mass murder. ( VOY : " Equinox ")
- Regulation 7 , Paragraph 4: An officer must consider themselves under arrest, unless in the presence of the most senior fellow officers presently available, the officers must give satisfactory answer to those charges… ( TOS : " The Omega Glory ")
- Regulation 15 : Regulation that prohibited the transfer of weapons by Starfleet officers to other races without the approval of the Federation Council . ( LD : " Second Contact ")
- Regulation 17.43 : In the alternate reality, this regulation related to Starfleet's ethical code of conduct, and was part of the Starfleet Code. Starfleet Academy cadets found cheating were accused to be in violation of the regulation. ( Star Trek )
- When an imminent threat was detected
- When the lives of Federation citizens were in danger
- When no other officers of equal or higher rank were present to mitigate the threat. ( DIS : " Brother ", PIC : " The Last Generation ")
- Regulation 25 : Regulation that prohibited the transfer of weapons by Starfleet officers to other races without the approval of the Federation Council. ( LD : " Second Contact ")
- Regulation 42/15 : "Pressure Variances in IRC Tank Storage". Part of the basic operational specifications for impulse engines, written by Montgomery Scott . The tanks could actually handle more pressure than the regulations allowed – in 2369, Geordi La Forge cited it as part of the impulse specifications while he and Scott worked to make the USS Jenolan operational, at which point Scott, realizing that he was thinking of this regulation, assured him that, as its author, he knew the tanks could be more efficient, but that La Forge should " Forget it. I wrote it; a good engineer is always a wee bit conservative… at least on paper. " ( TNG : " Relics ")
- Regulation 46A : If transmissions were being monitored during battle, no uncoded messages were to be transmitted on an open channel. ( Star Trek II: The Wrath of Khan )
- Regulation 76 : Prohibited pointing a phaser at a fellow Starfleet officer without a valid reason. ( LD : " Second Contact ")
- Regulation 157 , Section 3, Paragraph 18: Starfleet officers were required to take all necessary precautions to minimize any participation in historical events . ( DS9 : " Trials and Tribble-ations "; DIS : " Such Sweet Sorrow, Part 2 ")
- Regulation 191 (Article 14): In a combat situation involving more than one ship, command fell to the vessel with tactical superiority, should there not be a higher ranking officer present. ( VOY : " Equinox "; ST : " Ask Not ")
- Regulation 208 , Paragraph 2: Allowed an active captain to override the orders of other officers. Captain Christopher Pike cited this regulation to Cadet Thira Sidhu during a simulation in which he had supposedly been relieved of duty, and Cadet Sidhu had been ordered to keep him prisoner. Sidhu refused, pointing out that the regulation applied only to an active captain. ( ST : " Ask Not ")
- Regulation 256.15 : Starfleet officers shall display behavior befitting an officer at all times. ( DIS : " Far From Home ")
- Regulation 498 : Regulation that prohibited the transfer of weapons by Starfleet officers to other races without the approval of the Federation Council. ( LD : " Second Contact ")
- Regulation 619 : The commanding officer was required to relieve themselves of command if their current mission left them emotionally compromised and unable to make rational decisions. In 2258 of Nero 's alternate reality , when, after the destruction of Vulcan , Spock met a young James T. Kirk , marooned by this timeline's Spock , before returning him to the USS Enterprise , he told Kirk to use this regulation in order to take command of the ship. The elder Spock's advice was motivated by knowing that the conservative course his younger self would take would doom Earth to the same fate as Vulcan, while the unorthodox strategy Kirk would follow just might save it. Kirk succeeded in provoking Spock and he resigned command, but acted as Kirk's first officer afterwards, during the Battle of Earth . ( Star Trek )
- Regulation 756 : Regulation that prohibited the transfer of weapons by Starfleet officers to other races without the approval of the Federation Council. ( LD : " Second Contact ")
- Regulation 2884.3 : Substances unstable in an oxygen atmosphere were required to be handled with care. ( TNG : " Night Terrors ")
- Regulation 3287.0 : Due to its high volatile nature, antimatter was required to be stored in magnetic confinement pods . ( TNG : " Night Terrors ")
- Regulation 13982 : Allowed a Starfleet captain to conscript almost any person into service during a time of war. ( DIS : " Choose Your Pain ")
- Regulation 614617 : Prohibits permanent DNA modification. ( SNW : " Ad Astra per Aspera ")
- Reserve activation clause : A "little known" and "seldom used" clause in Starfleet regulations which allowed for the recall of a retired or discharged officer in the event of an emergency. ( Star Trek: The Motion Picture ; ST : " Ask Not ")
- Starfleet Rules of Conduct had some power to influence the operation of civilian establishments on Starfleet-administered installations, such as Quark's bar on Deep Space 9. ( DS9 : " Emissary ")
- The Starfleet uniform code governed the proper wearing of the uniform by Starfleet officers.
Starfleet Away Team Guidelines [ ]
- Section 12 , Paragraph 4: Related to the captain undertaking command of an away mission. During his best man speech at the wedding of William T. Riker and Deanna Troi in 2379 , Jean-Luc Picard stated that Commander Data would never let him undertake an away mission; Data reacted to that by reciting this regulation but was told to "shut up" by Picard before he could complete his sentence. ( Star Trek Nemesis )
- Regulation 476.9 : All away teams were required to report to the bridge at least once every twenty-four hours. ( VOY : " Once Upon a Time ")
- Medical Emergency on Alien Terrain : " It is recommended to keep an open com-channel at all times. " ( VOY : " Macrocosm ")
- " Specifically forbid the transport of unknown infectious agents onto a starship without establishing containment and eradication protocols. " ( VOY : " Macrocosm ")
- Unnumbered protocol : " Starfleet protocol demands that away teams remain armed and ready to defend themselves until contact is made. " ( VOY : " Tattoo ")
- Unnumbered protocol : Away teams must be composed of more than one crew member. Both Kathryn Janeway and Lieutenant Commander Tuvok cited this protocol to Seven of Nine when conducting an away mission. ( VOY : " Hunters ")
- Unnumbered regulation : Regulation that stated that the captain and first officer could not be on an away mission at the same time. In the alternate reality, Spock told acting captain James Kirk that he would cite this regulation when Kirk volunteered to beam to the Narada with him but did not do so because he knew Kirk would ignore it. ( Star Trek ) This regulation was also ignored when both Captain Kathryn Janeway and Commander Chakotay were infected with an unknown virus which inhibited their return to Voyager after an away mission. This resulted in both crew members being isolated on a planet in the Delta Quadrant and Lieutenant Tuvok being left in command of Voyager . ( VOY : " Resolutions ")
Starfleet Equipment Protocols [ ]
- SFRA 543447-87 . A photon warhead label mandates the observance of this protocol prior to the servicing or removal of the warhead. ( DS9 : " Tribunal ", label reference )
Starfleet Intelligence Procedures [ ]
- Luther Sloan , posing as Deputy Director of Starfleet Intelligence 's Department of Internal Affairs , cited standard containment procedures to isolate the senior staff , which included being relieved of duty and confined to quarters . ( DS9 : " Inquisition ")
Starfleet Medical Protocols [ ]
- Regulation 121 (Section A): The chief medical officer has the power to relieve an officer or crewman of his or her duties (including one of superior rank) if, in the CMO's professional judgment, the individual is medically unfit, compromised by an alien intelligence, ( TNG : " Lonely Among Us ") or otherwise exhibits behavior that indicates seriously impaired judgment. A Starfleet officer can face court martial for failing to submit to such a relief. In an alternate timeline generated by the Krenim , Captain Kathryn Janeway was relieved of her duties under this regulation by Voyager 's EMH, who had been observing reckless behavior on her part for weeks and attributed it to Traumatic Stress Syndrome . Janeway refused to surrender her duties, as she felt her efforts to bring her crew home were of more importance. Since security personnel had abandoned the ship, the EMH had no means of enforcing the regulation anyway. Janeway's actions later resulted in the erasure of this timeline, so the issue was non-existent. ( VOY : " Year of Hell, Part II ") In 2375 , aboard the Silver Blood Voyager , Neelix became, unofficially, chief medical officer after the loss of The Doctor. He threatened, in a lighthearted manner, to use his "authority" to relieve Janeway of her duties when she insisted on remaining in command although fatigued . ( VOY : " Course: Oblivion ")
- Unnumbered protocol : A physician must be present when administering arithrazine . A captain, when acting in accordance with the Omega Directive, could override this protocol. ( VOY : " The Omega Directive ")
See also [ ]
- Medical code
Starfleet Safety Protocols [ ]
- Safety Directive 3984/A . This regulation prohibited the use of ultritium 283 in class K planetary environments or in cryogenic substrates. This directive was updated on stardate 43094.3 . ( TNG : " Night Terrors ")
- SFRA 2884.3 . This regulation listed safety regulations for the use of balter compound 298 and tri-nickolas powder in a class N (2) planetary environment. ( TNG : " Night Terrors ")
- SFRA 3287.0 . This regulation stipulated that antimatter , and its derivative antideuterium , should be stored in magnetic containment pods . ( TNG : " Night Terrors ")
- SFRA 3842 . This regulation was associated with the antimatter injection system startup and operations in the engineering logs of the USS Enterprise -D . ( TNG : " Galaxy's Child ")
- SFRA 3843 . This regulation was associated with both the magnetic containment degauss protocol and antimatter safety procedures in the engineering logs of the USS Enterprise -D. ( TNG : " Galaxy's Child ")
- SFRA 3848 . This regulation established precautions for the use of industrial infusion charge applications in hypergravity and microgravity environments. ( TNG : " Night Terrors ")
- SFRA 3907A . This regulation was applicable for all uses of Walkerite 342 . ( TNG : " Night Terrors ")
- SFRA 3983 . This regulation prohibited the use of ultritium 283 in class K planetary environments or in cryogenic substrates. ( TNG : " Night Terrors ")
- SFRA 4832.4 . This regulation, which required compliance, described the proper handling and use of antideuterium. ( TNG : " Night Terrors ")
- SFRA 5443 . This regulation, which required compliance, legislated the use of the Lichfield suspension . ( TNG : " Night Terrors ")
- SFRA 8334A . This regulation was applicable for all uses of sternbachium . ( TNG : " Night Terrors ")
- SFRA 9323.4 . This regulation prohibited the use of bio-genovesium in biosynthetic food processing. ( TNG : " Night Terrors ")
- SFRA 43940 . This regulation was applicable for all uses of sternbachium. ( TNG : " Night Terrors ")
- SFRA 84349 . This regulation was applicable to all space vehicles, including the use of propellant for the ullage thruster devices and vernier thruster devices . ( TNG : " Night Terrors ")
- SFRA 83329.6 . This regulation recommended that Grant thermite 893 should be protected from ionizing radiation . ( TNG : " Night Terrors ")
- Unnumbered protocol . Tuvok once claimed that use of the transporters while at warp was a direct violation of Starfleet safety protocols. He did not cite the protocol by number, though the reason for caution was cited as having to do with the speed differential between two vessels. ( VOY : " Maneuvers ")
Starfleet Security Protocols [ ]
- Protocol 28 , Subsection D: " In the event of hostile alien takeover, the EMH is to deactivate and wait for rescue. " ( VOY : " Message in a Bottle ")
- Protocol 49.09 : Pertained to the treatment of prisoners on board a starship. In the alternate reality, Spock marooned James T. Kirk on Delta Vega . Kirk believed this act to be a violation of this protocol. ( Star Trek ) In 3188 , Saru cited this protocol to Osyraa regarding the presence of Ryn on board the USS Discovery . ( DIS : " The Sanctuary ")
- Unnumbered protocol : Luther Sloan, posing as deputy director of the Department of Internal Affairs, mentioned there was a security protocol that prevented others talking to prisoners under his authority without his clearance. ( DS9 : " Inquisition ")
Starfleet Temporal Protocols [ ]
Applicable in the event a Starfleet officer stranded in the past:
- No interfering with past events.
- No sharing knowledge of future. ( SNW : " Those Old Scientists ")
Starfleet Transfer Regulations [ ]
According to Leonard McCoy , the captain of a Starfleet vessel had the authority to transfer officers as he pleased, something which could be found in "a hundred volumes of space regulations somewhere." ( TOS : " The Conscience of the King ") Specific regulations were as follows:
- SFR-02-0933-3440 : Transfer of an Officer to Another Starship
- SFR-02-0933-3462F : Transfer Authority of a Starbase-Commanding Admiral (see graphic below)
- SFR-02-0933-3459C : Eligibility of Starfleet Exploratory Corps Personnel to Serve in Other Starfleet Divisions (see graphic below)
- SFR-02-9384-8896 : Transfer of Attached Scientific Personnel to Starship Duty
- SFR-02-8431-4933 : Authority for Assignment of Deep Space Exploratory Corps Personnel
- SFR-03-3823-3893 : Assignment of Starfleet Operational Support Officers
- SFR-03-8532-3892 : Emergency Assignment of Scientific and Research Specialists
- SFR-03-4832-3843 : Notification Requirements for Reassignment Within Deep Space Corps
- SFR-03-5931-0943 : Transfer of Starfleet Diplomatic Corps Personnel to Deep Space Duty
- SFR-04-4833-9834 : Eligibility for Exploratory Corps Personnel to Starbase Assignment
- SFR-04-4930-0027 : Transfer Policies for Daystrom Institute Faculty Researchers
- SFR-05-3832-9322 : Special Environmental Support Provisions for Class-K Native Personnel
- SFR-05-3023-3893 : Equal Treatment for Zero-Gravity Native Personnel
- SFR-06-3893-3892 : Transfer of Starfleet Tactical Specialists to Starbase Service
- SFR-06-0039-2174 : Authority for Assignment of Operational Support Personnel
- SFR-06-8342-9322 : Special Authority for Federation Diplomatic Corps
")
Starfleet Treaty Protocols [ ]
- SFPS 34.3.34.6: On stardate 44322 , Captain Rudolph Ransom 's ship, when in hiding from a Klingon Bird-of-Prey in a T-Tauri type nebula , operated within treaty protocols as set in this regulation. ( VOY : " Equinox, Part II ")
Starfleet/Federation Codes [ ]
- Code 1-Alpha-Zero : Indicated a starship in distress. ( TNG : " Relics ")
- Code 1 : Signaled either a total or imminent disaster, a possible invasion, or indicated that the Federation was either currently or about to be engaged in open warfare with a hostile power. The code required all Starfleet personnel within the affected area to immediately assume tactical alert. It was also colloquially known as "Defense Alert", or a "Priority One Alert". ( TOS : " Errand of Mercy ", " The Trouble with Tribbles ", " The Alternative Factor ", PIC : " The Last Generation ")
- Code 47 : An ultra-secure communications protocol, for captain's eyes only. This code was so secure that all traces of a Code 47 transmission or communication were automatically wiped from all computer records. ( TNG : " Conspiracy ")
- Code 710 : A "quarantine code". No Starfleet- or Federation-registered starship was to approach a system or vessel which was broadcasting Code 710. ( TOS : " A Taste of Armageddon ")
- Transporter Code 14 : A transporter procedure used to destroy an object.
Regulations not specified by name or number [ ]
Health-related [ ].
- " All research personnel on alien planets are required to have their health certified by a starship surgeon at one-year intervals. " ( TOS : " The Man Trap ")
- " The ship's surgeon will require a full examination of any crew member that he has doubts about, including the captain. " ( TOS : " Turnabout Intruder ")
- " Nothing shall be beamed aboard until danger of contamination has been eliminated. Beaming down to the surface (of a planet) is permitted, if the captain decides the mission is vital, and reasonably free of danger. " ( Star Trek III: The Search for Spock ; VOY : " Macrocosm ")
- A captain cannot order a doctor to violate doctor-patient confidentiality , except in situations of ship security. ( VOY : " Fury ")
- An officer taking medical leave could select their rehabilitation facility. ( DS9 : " It's Only a Paper Moon ")
- " The transport of a patient is to be performed at the discretion of the attending physician. " In 2258 of the alternate reality, Leonard McCoy , citing this, was allowed to bring Cadet James T. Kirk, suspended from duty, along to his posting aboard the Enterprise , as Kirk was quite visibly suffering from the symptoms of a Melvaran mud flea bite. In truth, McCoy himself was responsible for this, having infected Kirk precisely because he would then have the authority to bring his grounded friend aboard the ship. ( Star Trek )
Relationships [ ]
- During the 22nd century, individuals were not allowed to have sexual relations with colleagues, according to Starfleet regulations. ( ENT : " Bounty ")
- By the 23rd century, the above rule was either abolished completely, or replaced by protocols regarding fraternizations, which did not forbid romance, but may have required notifying Starfleet of such happening. The reasoning for such protocol was that Starfleet ran on command hierarchy, and fraternizations could lead to complications. ( SNW : " Lost in Translation ") It is unknown if such protocol continued in later eras.
- " All Starfleet personnel must obtain authorization from their CO as well as clearance from their medical officer before initiating an intimate relationship with an alien species. " ( VOY : " The Disease ")
- Culber and Stamets were married and shared Quarters during their time on USS Discovery .
- Leonard McCoy told Kirk that "there aren't any regulations against romance". ( TOS : " Space Seed ")
- Starfleet senior officers officiated various weddings between two crew members on board an active Starfleet ship. ( TOS : " Balance of Terror "; SNW : " A Quality of Mercy "; TNG : " Data's Day "; VOY : " Drive ")
- In 24th century, Picard mentioned to Deanna Troi that " there are no Starfleet regulations about a captain becoming involved with a fellow officer ". ( TNG : " Lessons ")
- William T. Riker and Troi continued to serve aboard the Enterprise and later the USS Titan , even after being married. ( Star Trek Nemesis ).
- Non-romantic, consensual sexual relationship/activity was implied to take place often on USS Cerritos , with its holodecks being the most common place for such to take place.
- By the 24th century, some duties may even have recommend the use of married couples, which could cause problems should the assigned ship not have such a couple. ( LD : " Parth Ferengi's Heart Place ")
Miscellaneous [ ]
- Again, this regulation may have been repealed/amended as there are many recorded instances of captains doing this.
- Removing an individual from a planet against their will violated several regulations, including the Prime Directive. Data reminded William T. Riker of this, who was considering rescuing a group of dissidents of Angel I from execution. They insisted on staying, even if this meant being executed . ( TNG : " Angel One ")
- " Striking a fellow officer is a court-martial offense. " ( ENT : " Bound "; TOS : " This Side of Paradise "; VOY : " Parallax ")
- 23rd century Starfleet captains had a high degree of authority on board the ship they were assigned to command. In extremes, a captain could invoke their "personal authority as captain" to order their subordinates to override the orders of a senior officer, even if the captain was not actually on board ship at the time. Such an order would almost certainly result in at least an inquiry after the crisis had passed. Captain Kirk used his "personal authority" to overrule the orders of Commodore Matt Decker and to have Spock resume command of the Enterprise during a battle with the planet killer . ( TOS : " The Doomsday Machine ")
- Starfleet regulations called for declaring a yellow alert when a starship was targeted by laser weapons . According to Jean-Luc Picard, such regulations were "very old". ( TNG : " The Outrageous Okona ")
- Protocols on first contact were available to Starfleet personnel, which was once revised by Captain McCoullough . ( DS9 : " Move Along Home ")
- According to Starfleet protocol, "sir" was the proper address when responding to one's commanding officer (or possibly any superior officer ), though some female officers, such as Kathryn Janeway , preferred "ma'am". ( VOY : " Caretaker ") Naval tradition dictated the use of "captain" for a ship's CO, regardless of the CO's rank. ( DS9 : " Behind the Lines ")
- Starfleet rules forbade dealing with outlaws and getting involved in the politics of other cultures. ( VOY : " Alliances ")
- Starfleet's policy was to deal with new species on a basis of openness and trust until proven otherwise. ( VOY : " Alliances ")
- Starfleet protocols included guidelines on proper punctuation of reports, such as conn reports . ( VOY : " Dreadnought ")
- " Encroaching on the territory of an alien species is prohibited. " ( VOY : " The Swarm ")
- " Ground combat personnel are to rotate off the front lines every ninety days. " ( DS9 : " The Siege of AR-558 ")
- " Interference in alien conflicts is strictly prohibited. " ( VOY : " Nightingale ")
- Procedures pertaining to official requests for asylum to a Starfleet captain included a hearing. ( VOY : " Death Wish ")
- Accidents aboard Starfleet vessels were to be followed by an investigation into the cause of the accident. ( VOY : " Day of Honor ")
- An official/formal letter, written to a senior officer , was required to be replied to by a senior officer. If the letter was to a vessel's captain, they could delegate the task of writing the response to their first officer or chief of security. ( VOY : " Tinker Tenor Doctor Spy ")
- Ensign Harry Kim referred to privacy protocols being violated by Lieutenant Commander Tuvok while the latter was investigating an attack on Ensign Tabor and read a letter that Harry's cousin , Dennis , had sent from Earth. Tuvok stated that, as chief of security , he had authority to suspend the protocols under special circumstances. ( VOY : " Repression ")
- Romulan whiskey was not allowed aboard Starfleet facilities. ( LD : " Second Contact ")
- Protocol allowed a Federation captain to grant political asylum in extreme circumstances. ( DIS : " The Examples ")
Fictional [ ]

Jean-Luc Picard quoting Starfleet Regulation 6.57 to Radue
- Regulation 6.57 : At least two staff officers were to be present during any treaty or contract negotiations. In 2364 , Jean-Luc Picard quoted this regulation to Radue of the Aldeans , who had recently kidnapped a group of specially gifted children from the Enterprise , offering scientific knowledge as compensation. Moments later, when Data admitted not to be familiar with the regulation, Picard revealed that it was, in fact, non-existent; it was merely something he had made up on the spot in order to deceive the Aldeans to allow him to bring Beverly Crusher with him to their planet 's surface. ( TNG : " When The Bough Breaks ")
- Tactical Directive 36A: B'Elanna Torres made up Tactical Directive 36A in 2377 , claiming that there should also be an engineer with the captain and not just a tactical officer . ( VOY : " Unimatrix Zero ")
- Directive 927 : " Always help those in need. " This directive was quoted by Dala as being part of the "Starfleet General Order" when she was posing as Kathryn Janeway, in 2376 . ( VOY : " Live Fast and Prosper ")
Appendices [ ]
Background information [ ].
As referred to in the revised final draft script of TOS : " Court Martial ", " Regulations 7, Subsection D " related to courts martial. It did not allow the defense to call a witness to provide testimony prior to the prosecution resting its case. The regulation was cited by Areel Shaw during Kirk's court martial at Starbase 11 .
In the revised final draft script of TNG : " Evolution ", " Protocol 'B' " was said to regulate how crew members could access all power components on a starship if they were no longer deemed reliable.
The Star Trek Encyclopedia (4th ed., vol. 2, p. 180) has a picture of a prop made for Admiral Pike 's office in Star Trek Into Darkness . This prop has text for the first three Starfleet General Orders. The prop might or might not have appeared in the film. These general orders were written by Chris Gray and modified by Chris St. John. [1] The text was slightly edited by the individual who made the prop for the film.
- General Order #2 was a prohibition against the use of unnecessary force: No Starfleet personnel shall unnecessary use force, either collectively or individually, against members of the United Federation of Planets, their duly authorized representatives, spokespersons, or designated leaders, or members of any sentient member race, for any reason whatsoever.
- General Order #3 was on the rights of the individual: The sovereignty of each Federation member being respected in all things, Starfleet personnel shall observe any or all statutes, laws, ordinances, and rules of governance currently in effect within the jurisdiction of a member world. Violators of such ordinances will be subject to such punishments or corrections as shall be determined by local governmental bodies.
"The only death penalty" [ ]
Varying statements about the status of the death penalty in the Federation and General Orders regarding it have been given in the Star Trek canon. Notably, at different times both General Order 4 and General Order 7 were said to be the only death penalty left.
" The Menagerie, Part I ", set in 2267 , introduced general order 7 as "the only death penalty left on our books". As it was specific to Talos IV , it was presumably instituted after Captain Pike 's 2254 mission to the planet. However, in " Turnabout Intruder ", set in 2269 , Sulu stated " The death penalty is forbidden. There's only one exception ", which turned out to be general order 4 (the nature of which remains unspecified).
Further complicating the situation, in DIS : " Si Vis Pacem, Para Bellum ", Admiral Katrina Cornwell explained Starfleet's policy on prisoners of war to L'Rell , stating that "the Federation has no death penalty". This episode is set in late 2256 or early 2257 , after Pike's visit to Talos IV but before "The Menagerie", thus making it unclear as to when the death penalty for visiting Talos IV was established. In DIS : " If Memory Serves ", the planet was said to be off limits, and the Discovery crew faced disciplinary action after visiting it, but no mention was made of General Order 4 or the death penalty.
Regarding the two General Orders each stated to be the only death penalty, if relations with the Talosians had not changed, it could be that one of the two General Orders might have been made to include other planets which might be a threat to the Federation like Talos IV . It is also possible that, in "Turnabout Intruder", Chekov misspoke. In the PC game Star Trek: 25th Anniversary , the USS Enterprise computer states that General Order 4 is sometimes confused with General Order 7 and the death penalty associated with it more generally refers to high treason.
Apocrypha [ ]
- Starfleet Catastrophic Response Code, Section A : When all forms of communication failed to establish a link between Starfleet vessels and any Federation outpost, all personnel and ordnance were required to attempt immediate rendezvous at Starfleet Command . ( Star Trek: First Frontier )
- General Order 16 : All Starfleet ships detecting the energy signature from one of four Malkus Artifacts were under orders to find and confiscate the artifacts. ( Star Trek: The Brave and the Bold )
- General Order 34 : Starfleet captains must honor, respect, and display extreme tolerance for species-based customs and practices insofar as the safety of the vessel was not threatened by such practices. ( Star Trek: New Frontier novel Being Human )
- Regulation 121 : An emotionally compromised officer was not fit to serve in the position of captain. ( Star Trek novelization )
- Regulation 1186, section 20 : The accepting of gifts on an individual basis by an official member of a formal diplomatic representation is strictly forbidden. ( Star Trek novel The Unsettling Stars )
- UFP Regulation 342-188564.3 , Paragraph 3: A class-3 biohazard alert. All personnel not part of a Biohazard Response Team were to stay away from any site broadcasting such an alert. ( Star Trek: 25th Anniversary , Episode 3: "Love's Labor Jeopardized")
- Secret Regulations of Stardate 7500 : The exact language was not specified, but the Secret Regulations of Stardate 7500 were outlined as the response to an invasion of the Federation. They were created on stardate 7500, amended stardate 42799, and gave the officer who invoked them the authority to second any Starfleet officers to their command and seniority in command decisions related to the invaders. In 2270 , under the authority of Starfleet General Order Three, Commander Riker invoked the secret regulations in response to the threat of an invasion by an alliance of the Borg Collective and a breakaway faction of the Romulan Star Empire . ( Star Trek: The Return )
- Starfleet Protocol 547c : Not really known, but seeing as it was cited while trying to shut down force fields leading to the USS Enterprise -C , it is assumed that it was a security protocol. It was cited as an utterance by an annoyed Tasha Yar when she realized there was a group of force fields that had been missed when shutting down security. Frustrated, Richard Castillo griped that the Tholians had most likely never heard of Protocol 547c. ( Star Trek Online , "Temporal Ambassador")
- General Order 24, mentioned in TOS : " Whom Gods Destroy " and " A Taste of Armageddon " as allowing for the destruction of all life on a planet, was actually carried out in the first issue of the Gold Key Star Trek comic series " The Planet of No Return ", and the novel Reap the Whirlwind in the Star Trek: Vanguard series.
- Starfleet Regulation 320-730-A, Subparagraph 2 : Knick-knack shelves were not mandatory for Starfleet captains, but if they did have one, it was required to have at least one (1) " little ship ". ( Star Trek: Lower Decks, Issue 1 )
- Terran General Order Four
External link [ ]
- Starfleet General Orders and Regulations at Memory Beta , the wiki for licensed Star Trek works
- 3 Ancient humanoid
IMAGES
VIDEO
COMMENTS
The following is a list of medical procedures. See also: Medical conditions and illnesses Medical equipment Medicinal drugs and treatments. Memory Alpha. Explore. Main Page; Discuss; All Pages; ... Star Trek; Into Darkness; Beyond; XIV; Undeveloped. Phase II; Planet of the Titans "Kirk Meets JFK" The First Adventure; The Beginning; Star Trek 4 ...
Star Trek's biobeds also double up as operating tables for surgical procedures, with life sign scanners, a wraparound bank of sensors, and attachments for medical equipment. Larger surgical biobeds were used for more invasive surgery like the controversial genetronic procedure that reversed the paralysis suffered by Lt. Worf (Michael Dorn) in ...
Paramount and the creators of Star Trek do not endorse, sanction, or authorize any material presented. 2 Contents Page Number(s) Front Cover 1 Table of Contents 2 ... Medical Procedures 25-26 STARFLEET Medical Protocols 27-28 Commonly Used Medications 28-38 Common Illnesses and Diseases 38-41
The Emergency Medical Holographic program (EMH) was formally known as an "EMH Program AK-1 Diagnostic and Surgical Subroutine Omega-323", though Zimmerman wanted to call his creation the "Holo-Doc", but Starfleet Command made the request to name the hologram "Emergency Medical Hologram" instead. ( VOY: " Projections " ) The persona was not ...
A DNA Reference Scan was a medical procedure to identify an individual by matching the DNA patterns with those on file. ... Image: Medical Tricorder, from Star Trek Adventures, Science Division Rulebook. The medical tricorder was a specialized version of the standard tricorder. It was equipped with sensors and analysis software tailored for ...
ESU Lab. When Theodore Maiman successfully fired the first laser in 1960, just six years before Star Trek first aired, people almost immediately recognized its potential uses as a surgical tool. In theory, by focusing energy towards a specific place, lasers should allow a surgeon to make precise cuts even in hard-to-reach areas of the body.
We hope you enjoy this new Replicator Resource. We hope it saves the lives of your valuable PCs and brings out your inner Dr. McCoys. Star Trek Adventures - Medical Reference Guide. PDF VERSION: STA -MEDICAL REFERENCE GUIDE. When asked to brag about himself, contributor Jason Marden said, "Hi, I'm Jase but you might know me as Hairy Gamer ...
an interest in the Medical Branch concept of Star Trek as it is applied by the SFMC. It is intended to serve as a handy reference work for members of the Medical ... of medical reference. While the procedures and protocols in this techniques are based on real-life medicine, it is not meant to be performed by personnels without ...
3 Appendix A: Star Trek Illnesses. 4 Appendix B: Star Trek Medical Scans, Tests, and Screenings. 5 ...
Published Mar 10, 2020. Star Trek has always featured wondrous pieces of technology, and the Emergency Medical Holographic (EMH) program is one of the most intriguing. In the newest Star Trek series, Picard, one of the most fascinating thing going on in the background are Rios' holographic programs. Since he runs this ship on his own, without ...
Star Trek: 23rd century medicine vs. 20th century medicine. Perhaps the most amusing example of McCoy's contempt for the "primitive" medicine of the 20th century occurs in the 1986 movie Star Trek IV: The Voyage Home. (I found it particularly amusing because I was a third year medical student when the movie came out.)
A medical device or medical supply was a form of medical technology intended for use to diagnose, treat, cure or prevent disease or other conditions in lifeforms. Where medical equipment was designed to aid in the diagnosis, monitoring or treatment of a medical conditions. Anti-grav lift Biobed Biological sample kit Cast Decompression chamber Emergency Medical Holographic program Holographic ...
The engine room has a lot of glamour, science-wise, and the bridge is always where the action is — but dating back to the days of Leonard McCoy, sickbay is also a key part of any interstellar (ahem) enterprise, and it's no stranger to Star Trek's spooky ability to predict future technology. The classic Trek series had its biobeds, and ...
Doctors are important characters in Star Trek. After a disaster that strands the starship Voyager on the other side of the galaxy and kills all of the medical personnel, the ship is forced to rely solely on the Emergency Medical Hologram, a sentient piece of holographic technology. The EMH is programmed with all known medical knowledge making ...
In the case of medical technology, the long-running TV and film series Star Trek has increasingly been inspiring researchers worldwide. Two teams were recently awarded the Qualcomm Tricorder X ...
Subspace. In the Star Trek fictional universe, subspace is a feature of space-time that facilitates faster-than-light transit, in the form of interstellar travel or the transmission of information. Faster-than-light warp drive travel via subspace obeys different laws of physics. The name "subspace" has also been adopted and used in other fictional settings, such as the Stargate franchise, The ...
The runner-up technology from Taiwan's Dynamical Biomarkers Group similarly connects a smartphone to several wireless handheld test modules that can analyse vital signs, blood and urine, and ...
The following is a list of medical substances and treatments for various illnesses by usage. asinolyathin bicaridine hydrocortilene metorapan morphenolog terakine triptacederine anesthizine anetrizine axonol hyvroxilated quint-ethyl metacetamin melenex nasal numbing agent neurozine dermaline dermaline gel kelotane adrenaline anticoagulant benjisidrine digoxin lectrazine metrazene vasokin ...
The Chief medical officer (CMO) was a senior staff position and was responsible for the maintenance of a crew's health and fitness. In a Starfleet unit, the officer also served as chief surgeon. The chief medical officer maintained and operated medical facilities of starships, stations, and planetary posts. The medical staff, including all medical officers and counselors, were overseen by the ...
Christopher Collins' next Star Trek appearance came later in Star Trek: The Next Generation season 2 when he played Captain Grebnedlog, the commander of the Pakled ship Mondor.As Captain Picard heads to a nearby starbase for a medical procedure, Commander Riker is left in command of the USS Enterprise-D.
Actress Barbara Baldavin, who appeared in three episodes of the original "Star Trek" television series during its first season and later appeared on "Medical Center," died Sunday. She was 85.
Barbara Baldavin, Actress on 'Star Trek' and 'Medical Center,' Dies at 85. She later was involved in casting on such series as 'Dynasty,' 'Matt Houston' and 'Trapper John, M.D.'
The interior of the Starfleet Medical facility shown in "Broken Bow" was a redress of the set later used to represent Enterprise's armory (which was built for the episode but not used therein). ("Broken Bow" text commentary, ENT Season 1 DVD) In its Starfleet Medical guise, the set also included the glass from the EMH's office from Star Trek: Voyager ("Broken Bow" text commentary, ENT Season 1 ...
Ms. Harris may make for a more natural messenger on abortion than Mr. Biden, an 81-year-old practicing Catholic who has long expressed personal discomfort with the procedure even as he has become ...
General Order 1, Section 2. General Order 1: "No starship may interfere with the normal development of any alien life or society." (TAS: "The Magicks of Megas-Tu") In 2259, the Federation Council renamed General Order 1 the Prime Directive, a title by which it later became better known.(SNW: "Strange New Worlds"; TNG: "The Drumhead"; PRO: "First Con-tact") It superseded all other laws and ...